The Effect of Chemoradiotherapy with SRC Tyrosine Kinase Inhibitor, PP2 and Temozolomide on Malignant Glioma Cells In Vitro and In Vivo
- Affiliations
-
- 1Department of Radiation Oncology, Seoul National University, Graduate School of Medicine, Seoul, Korea. inah228@snu.ac.kr
- 2Medical Science Research Institute, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Department of Radiation Oncology, Seoul National University College of Medicine, Seoul, Korea.
- 4Cancer Research Institute, Seoul National University, Seoul, Korea.
- 5Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2454347
- DOI: http://doi.org/10.4143/crt.2014.320
Abstract
- PURPOSE
We investigated the effect of chemoradiotherapy with PP2 and temozolomide (TMZ) on malignant glioma cells using clonogenic assays and in vivo brain tumor model.
MATERIALS AND METHODS
The effect of PP2 on radiosensitivity of U251 and T98G cells was investigated using clonogenic assays. The expression of E-cadherin, matrix metalloproteinases 2 (MMP2), Ephrin type-A receptor 2 (EphA2), and vascular endothelial growth factor (VEGF) was measured by Western blotting and an accumulation of γH2AX foci 6 hours after radiotherapy was measured after PP2 treatment. The effect of PP2 on migration, invasion, and vasculogenic mimicry formation (VMF) of U251 cells was evaluated. In an orthotopical brain tumor model with U251 cells, PP2 was injected intraperitoneally with or without oral TMZ before, during and after whole brain radiotherapy. Bioluminescence images were taken to visualize in vivo tumors and immunohistochemical staining of VEGF, CD31, EphA2, and hypoxia-inducible factor 1a was performed.
RESULTS
PP2 increased radiosensitivity of U251 and T98G cells without decreasing survival of normal human astrocytes. Chemoradiotherapy with PP2 and TMZ resulted in increased accumulation of γH2AX foci. PP2 induced overexpression of E-cadherin and suppression of MMP2, VEGF, and EphA2. PP2 also compromised invasion, migration, and VMF of U251 cells. In brain tumors, chemoradiotherapy with PP2 and TMZ decreased tumor volume best, but not statistically significantly compared with chemoradiotherapy with TMZ. The expression of VEGF and CD31 was suppressed in PP2-treated tumors.
CONCLUSION
PP2 enhances radiosensitivity of malignant glioma cells and suppresses invasion and migration of U251 cells. Chemoradiotherapy with PP2 and TMZ resulted in non-significant tumor volume decrease.
MeSH Terms
-
Astrocytes
Blotting, Western
Brain
Brain Neoplasms
Cadherins
Chemoradiotherapy*
Glioblastoma
Glioma*
Humans
In Vitro Techniques*
Matrix Metalloproteinases
Protein-Tyrosine Kinases*
Radiation Tolerance
Radiotherapy
Tumor Burden
Tyrosine*
Vascular Endothelial Growth Factor A
Cadherins
Matrix Metalloproteinases
Protein-Tyrosine Kinases
Tyrosine
Vascular Endothelial Growth Factor A
Figure
-

Fig. 1. Clonogenic assays of U251 and T98G cells after treating PP2, temozolomide (TMZ), or both. Cell surviving curves after treating PP2 (10 μM), TMZ (25 μM), or both were generated. The points indicate the mean surviving fractions at each dose level (±standard error). The lines are fitted to linear-quadratic equations. An addition of PP2 to TMZ showed an additive cytotoxic effect both in U251 and T98G cells. Sensitizer enhancement ratios (SER) were defined as isoeffective dose at surviving fraction 0.5 or 0.05. PP2 induced radiosensitization in U251 and T98G cells irrespective of MGMT promoter methylation. EGFR, epidermal growth factor receptor; RT, radiotherapy.
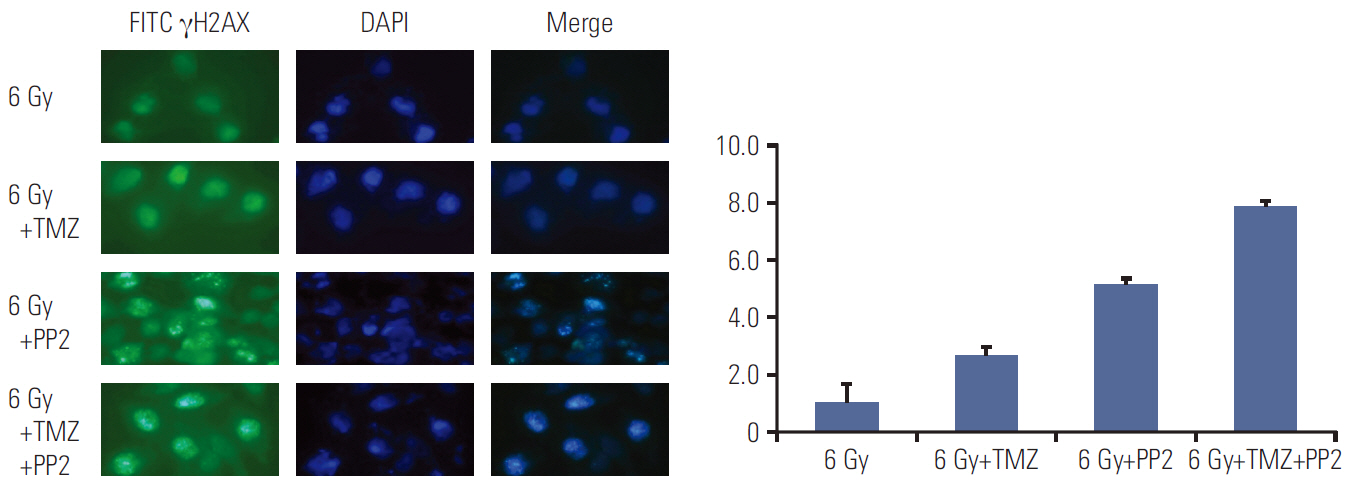
Fig. 2. Representative images of γH2AX foci formation in U251 cells. γH2AX foci formation was measured in U251 cells after treating PP2 (10 μM), temozolomide (TMZ, 25 μM), or both. The nuclei stained by DAPI are shown in blue, while the γH2AX foci stained by FITC are shown in green. Increased accumulation of γH2AX foci after treating PP2 and TMZ was confirmed by indirect immunofluorescence 6 hours after radiotherapy (6 Gy), indicating delayed DNA double strand breakage repair. All differences between the groups (6 Gy vs. 6 Gy+TMZ, p=0.014; 6 Gy+TMZ vs. 6 Gy+PP2, p=0.020; 6 Gy+PP2 vs. 6 Gy+TMZ+PP2, p=0.016) were statistically significant.
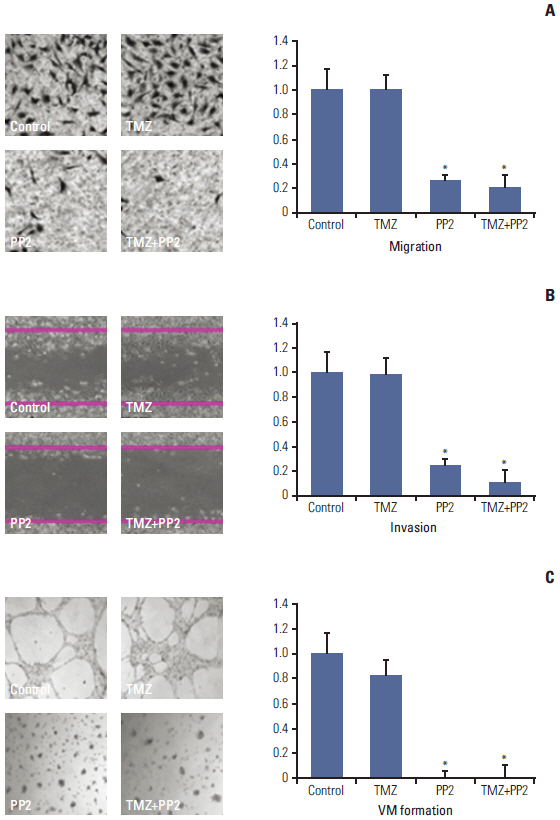
Fig. 3. Representative images of modified Boyden chamber assay (A), wound healing assay (B), and vasculogenic mimicry (VM) formation assay (C). (A) U251 cells were treated with PP2 (10 μM), temozolomide (TMZ, 25 μM), or both for 24 hours, and cell invasion was measured using a Transwell system with 8-μm pores in polycarbonate membranes. Results are expressed as a ratio of radiotherapy alone (control). (B) U251 cells were grown to confluence in 6-well plates and then starved for 24 hours. A linear scratch was made in each hemisphere of the well with 1-mL pipette tip. Images were taken of the intersections of linear cell wound and each grid line. (C) Two hundred microliters ECM Matrigel was dropped in 48-well tissue culture plates and then incubated at 37°C for 2 hours. Column, bar, and asterisk represent the mean of three independent experiments, standard error, and statistical significance of p < 0.05 when compared with control, respectively.

Fig. 4. Western blotting of U251 cells after treating inhibitors. After PP2 (10 μM) treatment, E-cadherin was overexpressed, while expression of matrix metalloproteinase 2 (MMP2), Ephrin type-A receptor 2 (EphA2), and vascular endothelial growth factor (VEGF) were suppressed. TMZ, temozolomide.

Fig. 5. The surviving fraction at 2 Gy (SF2) of X-ray in normal human astrocytes. SF2 was measured after treating PP2 (10 μM), temozolomide (TMZ, 25 μM), or both. The points indicate the mean surviving fractions at each dose level. Column and bar represent mean of three independent experiments and standard error, respectively.
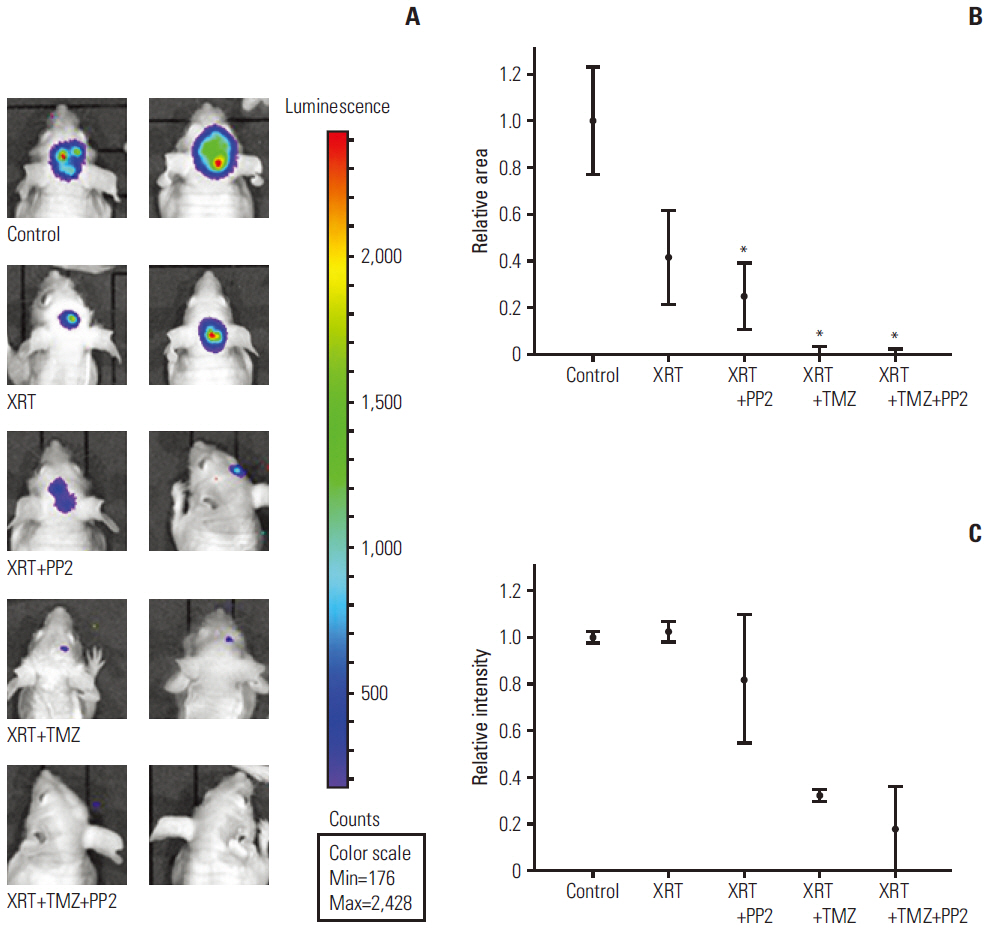
Fig. 6. (A) Representative bioluminescence images of human brain tumor xenograft in nude mice. U251 cells were injected orthotopically into thalamic area using a 26G needle with syringe. Bioluminescence images were obtained 7 days after injection, and then randomly assigned to control or experimental groups as follows: control, radiotherapy (XRT), XRT+PP2, XRT+temozolomide (TMZ), and XRT+TMZ+PP2, respectively. Chemoradiotherapy with TMZ exhibited marked tumor shrinkage and chemoradiotherapy with PP2 and TMZ led to non-visualization of tumors, indicating an additional radiosensitization by PP2. (B) In semi-quantitative analyses of relative luminescence area, combination of PP2 and TMZ resulted in a smaller area of luminescence than TMZ or PP2 alone, but it was not statistically significant. Bar represents standard error. (C) TMZ-treated groups had smaller mean intensity than control or radiotherapy alone. However, the difference between TMZ and PP2 plus TMZ group was not significant.
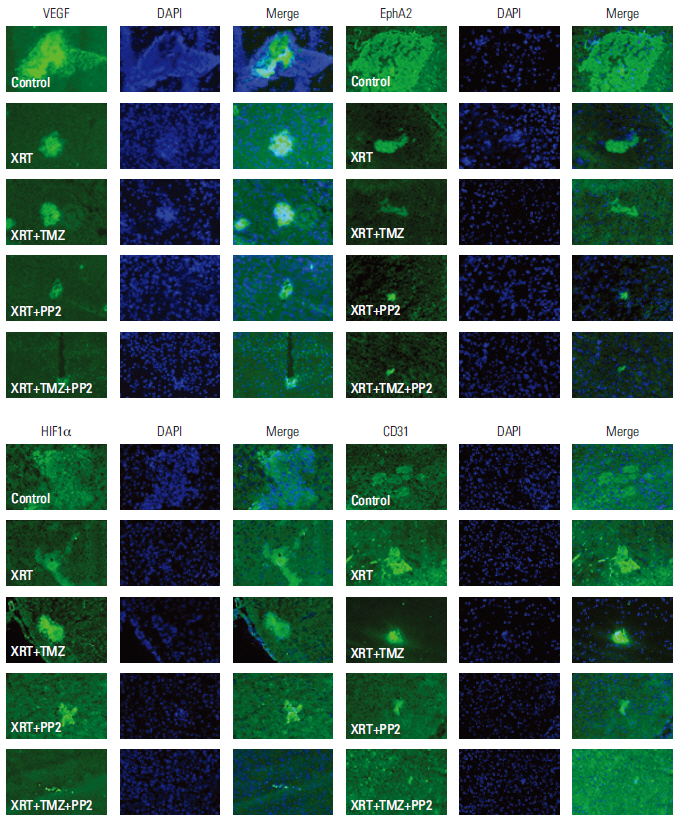
Fig. 7. Immunohistochemical stains of in vivo human brain tumors in nude mice. Immunohistochemical staining with antibodies against vascular endothelial growth factor (VEGF), CD31, Ephrin type-A receptor 2 (EphA2), and hypoxia-inducible factor 1α (HIF1α) was performed. The expression of VEGF and CD31 were down-regulated in PP2-treated tumors relative to those with XRT alone or XRT plus temozolomide (TMZ) tumors, suggesting that PP2 may suppress angiogenesis in in vivo tumor as well as in in vitro cells. Expression of EphA2 and HIF1α were not influenced by PP2 treatment in in vivo tumors. XRT, radiotherapy.
Reference
-
References
1. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005; 352:987–96.
Article2. Masui K, Cloughesy TF, Mischel PS. Review: molecular pathology in adult high-grade gliomas: from molecular diagnostics to target therapies. Neuropathol Appl Neurobiol. 2012; 38:271–91.3. Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005; 352:997–1003.4. Angers-Loustau A, Hering R, Werbowetski TE, Kaplan DR, Del Maestro RF. SRC regulates actin dynamics and invasion of malignant glial cells in three dimensions. Mol Cancer Res. 2004; 2:595–605.5. Stehelin D, Fujita DJ, Padgett T, Varmus HE, Bishop JM. Detection and enumeration of transformation-defective strains of avian sarcoma virus with molecular hybridization. Virology. 1977; 76:675–84.
Article6. Stettner MR, Wang W, Nabors LB, Bharara S, Flynn DC, Grammer JR, et al. Lyn kinase activity is the predominant cellular SRC kinase activity in glioblastoma tumor cells. Cancer Res. 2005; 65:5535–43.
Article7. Du J, Bernasconi P, Clauser KR, Mani DR, Finn SP, Beroukhim R, et al. Bead-based profiling of tyrosine kinase phosphorylation identifies SRC as a potential target for glioblastoma therapy. Nat Biotechnol. 2009; 27:77–83.
Article8. Ding Q, Stewart J Jr, Olman MA, Klobe MR, Gladson CL. The pattern of enhancement of Src kinase activity on platelet-derived growth factor stimulation of glioblastoma cells is affected by the integrin engaged. J Biol Chem. 2003; 278:39882–91.
Article9. Jallal H, Valentino ML, Chen G, Boschelli F, Ali S, Rabbani SA. A Src/Abl kinase inhibitor, SKI-606, blocks breast cancer invasion, growth, and metastasis in vitro and in vivo. Cancer Res. 2007; 67:1580–8.10. Park CM, Park MJ, Kwak HJ, Lee HC, Kim MS, Lee SH, et al. Ionizing radiation enhances matrix metalloproteinase-2 secretion and invasion of glioma cells through Src/epidermal growth factor receptor-mediated p38/Akt and phosphatidylinositol 3-kinase/Akt signaling pathways. Cancer Res. 2006; 66:8511–9.
Article11. Rothschild SI, Gautschi O, Haura EB, Johnson FM. Src inhibitors in lung cancer: current status and future directions. Clin Lung Cancer. 2010; 11:238–42.
Article12. Cuneo KC, Geng L, Tan J, Brousal J, Shinohara ET, Osusky K, et al. SRC family kinase inhibitor SU6656 enhances antiangiogenic effect of irradiation. Int J Radiat Oncol Biol Phys. 2006; 64:1197–203.
Article13. Kim IA, No M, Lee JM, Shin JH, Oh JS, Choi EJ, et al. Epigenetic modulation of radiation response in human cancer cells with activated EGFR or HER-2 signaling: potential role of histone deacetylase 6. Radiother Oncol. 2009; 92:125–32.
Article14. Lee KM, Choi EJ, Kim IA. microRNA-7 increases radiosensitivity of human cancer cells with activated EGFR-associated signaling. Radiother Oncol. 2011; 101:171–6.
Article15. Fischer AH, Jacobson KA, Rose J, Zeller R. Cryosectioning tissues. CSH Protoc. 2008; 2008:pdb.prot4991.
Article16. Chahal M, Abdulkarim B, Xu Y, Guiot MC, Easaw JC, Stifani N, et al. O6-Methylguanine-DNA methyltransferase is a novel negative effector of invasion in glioblastoma multiforme. Mol Cancer Ther. 2012; 11:2440–50.
Article17. Hanson JA, Hsu FP, Jacob AT, Bota DA, Alexandru D. Antivascular endothelial growth factor antibody for treatment of glioblastoma multiforme. Perm J. 2013; 17:68–74.
Article18. Wong ET, Gautam S, Malchow C, Lun M, Pan E, Brem S. Bevacizumab for recurrent glioblastoma multiforme: a meta-analysis. J Natl Compr Canc Netw. 2011; 9:403–7.
Article19. Huveldt D, Lewis-Tuffin LJ, Carlson BL, Schroeder MA, Rodriguez F, Giannini C, et al. Targeting Src family kinases inhibits bevacizumab-induced glioma cell invasion. PLoS One. 2013; 8:e56505.
Article20. Le DM, Besson A, Fogg DK, Choi KS, Waisman DM, Goodyer CG, et al. Exploitation of astrocytes by glioma cells to facilitate invasiveness: a mechanism involving matrix metalloproteinase- 2 and the urokinase-type plasminogen activator-plasmin cascade. J Neurosci. 2003; 23:4034–43.21. Wilkinson DG. Multiple roles of EPH receptors and ephrins in neural development. Nat Rev Neurosci. 2001; 2:155–64.
Article22. Wykosky J, Gibo DM, Stanton C, Debinski W. EphA2 as a novel molecular marker and target in glioblastoma multiforme. Mol Cancer Res. 2005; 3:541–51.
Article23. Zhou N, Zhao WD, Liu DX, Liang Y, Fang WG, Li B, et al. Inactivation of EphA2 promotes tight junction formation and impairs angiogenesis in brain endothelial cells. Microvasc Res. 2011; 82:113–21.
Article24. Zhuang G, Brantley-Sieders DM, Vaught D, Yu J, Xie L, Wells S, et al. Elevation of receptor tyrosine kinase EphA2 mediates resistance to trastuzumab therapy. Cancer Res. 2010; 70:299–308.
Article25. Holen HL, Shadidi M, Narvhus K, Kjosnes O, Tierens A, Aasheim HC. Signaling through ephrin-A ligand leads to activation of Src-family kinases, Akt phosphorylation, and inhibition of antigen receptor-induced apoptosis. J Leukoc Biol. 2008; 84:1183–91.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Involvement of Src Family Tyrosine Kinase in Apoptosis of Human Neutrophils Induced by Protozoan Parasite Entamoeba histolytica
- Fyn Tyrosine Kinase-mediated Tyrosine Phosphorylation of Roundabout (Robo), the Slit Receptor
- The Difference in Biological Properties between Parental and v-Ha-ras Transformed NIH3T3 Cells
- Mutant IDH1 Enhances Temozolomide Sensitivity via Regulation of the ATM/CHK2 Pathway in Glioma
- Src Family Kinase Inhibitor PP2 Has Different Effects on All-Trans-Retinoic Acid or Arsenic Trioxide-Induced Differentiation of an Acute Promyelocytic Leukemia Cell Line
