Korean J Urol.
2012 Apr;53(4):268-274.
Influence of Overweight on 24-Hour Urine Chemistry Studies and Recurrent Urolithiasis in Children
- Affiliations
-
- 1Department of Urology, Chung-Ang University College of Medicine, Seoul, Korea. caucih@cau.ac.kr
Abstract
- PURPOSE
We investigated the influence of overweight on 24-hour urine chemistry studies and recurrent urolithiasis (UL) in children.
MATERIALS AND METHODS
A retrospective cohort study was designed to assess children who presented with UL at a pediatric institution between 1985 and 2010. We calculated body mass index percentile (BMIp) adjusted for gender and age according to the 2007 Korean Children and Adolescents Growth Chart and stratified the children into 3 BMI categories: lower body weight (LBW, BMIp< or =10), normal BW (NBW, 10
RESULTS
A total of 125 patients were included. The age of the patients in the NBW group was older than that of patients in the LBW group, but 24-hour urine chemistry studies did not differ significantly between the three groups. Mean urine citrate levels were lower (0.273+/-0.218 mg/mg/d vs. 0.429+/-0.299 mg/mg/d, p<0.05) and the incidence of hypocitraturia was higher (81.5% vs. 45.7%, p<0.05)) in the recurrent stone former group. In the univariate analysis, hypocitraturia and acidic urinary pH were risk factors, but in the multivariate analysis, only hypocitraturia was a risk factor for stone recurrence (hazard ratio, 3.647; 95% confidence interval, 1.047 to 12.703). In the Kaplan-Meier curve, the hypocitraturia group showed higher recurrence than did the normocitraturia group (p<0.05).
CONCLUSIONS
Unlike in adults, in children, overweight adjusted for gender and age was not associated with 24-hour urine chemistry studies and was not a risk factor for recurrent UL. Hypocitraturia was the only risk factor for UL in children.
MeSH Terms
Figure
-
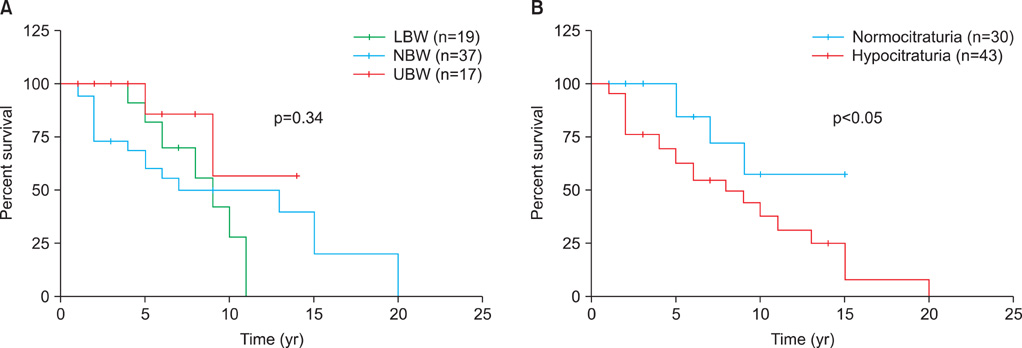
FIG. 1 Kaplan-Meier curve estimating the probability of stone recurrence according to patient age and body mass index percentile. LBW, lower body weight; NBW, normal body weight; UBW, upper body weight.
Reference
-
1. Vahlensieck W, Bach D, Hesse A. Incidence, prevalence and mortality of urolithiasis in West Germany. Helv Chir Acta. 1982. 49:445–449.2. VanDervoort K, Wiesen J, Frank R, Vento S, Crosby V, Chandra M, et al. Urolithiasis in pediatric patients: a single center study of incidence, clinical presentation and outcome. J Urol. 2007. 177:2300–2305.3. Milliner DS, Murphy ME. Urolithiasis in pediatric patients. Mayo Clin Proc. 1993. 68:241–248.4. Stapleton FB. Childhood stones. Endocrinol Metab Clin North Am. 2002. 31:1001–1015. ix5. Worcester EM, Coe FL. Nephrolithiasis. Prim Care. 2008. 35:369–391. vii6. Daudon M, Lacour B, Jungers P. Influence of body size on urinary stone composition in men and women. Urol Res. 2006. 34:193–199.7. Powell CR, Stoller ML, Schwartz BF, Kane C, Gentle DL, Bruce JE, et al. Impact of body weight on urinary electrolytes in urinary stone formers. Urology. 2000. 55:825–830.8. Taylor EN, Curhan GC. Body size and 24-hour urine composition. Am J Kidney Dis. 2006. 48:905–915.9. Peres LA, Langer SS, Schmidt RC, Nacke RA, Francescon PV, Almeida RC, et al. Nephrolithiasis in pediatric patients: metabolic and anatomical investigation. J Bras Nefrol. 2011. 33:50–54.10. The Committee for the Development of Growth Standard for Korean Children and Adolescents. The Committee for School Health and Public Health Statistics, The Korean Pediatric Society. Division of Chronic Disease Surveillance, Korea Center for Disease Control and Prevention. 2007 Korean Children and Adolescents Growth Standard (commentary for the development of 2007 growth chart). 2007. Cheongwon: Division of Chronic Disease Surveillance, Korea Center for Disease Control and Prevention.11. Taylor EN, Stampfer MJ, Curhan GC. Obesity, weight gain, and the risk of kidney stones. JAMA. 2005. 293:455–462.12. Semins MJ, Shore AD, Makary MA, Magnuson T, Johns R, Matlaga BR. The association of increasing body mass index and kidney stone disease. J Urol. 2010. 183:571–575.13. Siener R, Glatz S, Nicolay C, Hesse A. The role of overweight and obesity in calcium oxalate stone formation. Obes Res. 2004. 12:106–113.14. Li WM, Chou YH, Li CC, Liu CC, Huang SP, Wu WJ, et al. Association of body mass index and urine pH in patients with urolithiasis. Urol Res. 2009. 37:193–196.15. Jung HS, Chang IH, Kim KD, Moon YT, Kim TH, Myung SC, et al. Possible relationship between metabolic syndrome traits and nephrolithiasis: incidence for 15 years according to gender. Korean J Urol. 2011. 52:548–553.16. Chang IH, Lee YT, Lee DM, Kim TH, Myung SC, Kim YS, et al. Metabolic syndrome, urine pH, and time-dependent risk of nephrolithiasis in Korean men without hypertension and diabetes. Urology. 2011. 78:753–758.17. Lee SC, Kim YJ, Kim TH, Yun SJ, Lee NK, Kim WJ. Impact of obesity in patients with urolithiasis and its prognostic usefulness in stone recurrence. J Urol. 2008. 179:570–574.18. Sarica K, Eryildirim B, Yencilek F, Kuyumcuoglu U. Role of overweight status on stone-forming risk factors in children: a prospective study. Urology. 2009. 73:1003–1007.19. Kieran K, Giel DW, Morris BJ, Wan JY, Tidwell CD, Giem A, et al. Pediatric urolithiasis-does body mass index influence stone presentation and treatment? J Urol. 2010. 184:4 Suppl. 1810–1815.20. Kim SS, Luan X, Canning DA, Landis JR, Keren R. Association between body mass index and urolithiasis in children. J Urol. 2011. 186:4 Suppl. 1734–1739.21. Pietrow PK, Pope JC 4th, Adams MC, Shyr Y, Brock JW 3rd. Clinical outcome of pediatric stone disease. J Urol. 2002. 167(2 Pt 1):670–673.22. Spivacow FR, Negri AL, del Valle EE, Calviño I, Fradinger E, Zanchetta JR. Metabolic risk factors in children with kidney stone disease. Pediatr Nephrol. 2008. 23:1129–1133.23. Acar B, Inci Arikan F, Emeksiz S, Dallar Y. Risk factors for nephrolithiasis in children. World J Urol. 2008. 26:627–630.24. Tefekli A, Esen T, Ziylan O, Erol B, Armagan A, Ander H, et al. Metabolic risk factors in pediatric and adult calcium oxalate urinary stone formers: is there any difference? Urol Int. 2003. 70:273–277.25. DeFoor WR, Jackson E, Minevich E, Caillat A, Reddy P, Sheldon C, et al. The risk of recurrent urolithiasis in children is dependent on urinary calcium and citrate. Urology. 2010. 76:242–245.26. Dursun I, Poyrazoglu HM, Dusunsel R, Gunduz Z, Gurgoze MK, Demirci D, et al. Pediatric urolithiasis: an 8-year experience of single centre. Int Urol Nephrol. 2008. 40:3–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prevention and management of urinary stone
- Bone and Metabolic Markers in Women With Recurrent Calcium Stones
- Metabolic Abnormalities and the Risk for Recurrence in Obese Patients with Urolithiasis
- Metabolic Abnormalities of 24-hour Urinary Lithogenic Factors in Recurrent Stone Formers
- Comparison of Metabolic Risk Factors in Patients with 1st Episode Urolithiasis Stratified according to Age
