Korean J Urol.
2007 Jul;48(7):718-723. 10.4111/kju.2007.48.7.718.
Metabolic Abnormalities and the Risk for Recurrence in Obese Patients with Urolithiasis
- Affiliations
-
- 1Department of Urology, Chungbuk National University College of Medicine, Cheongju, Korea. lscuro@chungbuk.ac.kr
- KMID: 1990224
- DOI: http://doi.org/10.4111/kju.2007.48.7.718
Abstract
-
PURPOSE: Recent studies have suggested an increased prevalence of urolithiasis with obesity. This study aimed to assess the influence of obesity on urinary metabolic abnormalities and the recurrence of stone.
MATERIALS AND METHODS
We analyzed 802 consecutive stone formers(SF: first-time SF=501, recurrent SF=291) who underwent a comprehensive metabolic evaluation that included blood chemistry tests and a 24-hour urinary examination, as well as determining the body mass index(BMI). The BMI was categorized into the non-obese(BMI<25kg/m2) and obese(BMI>or=25kg/m2) according to the re-defined Western Pacific Region WHO criteria on obesity(WPRO). All possible risk factors such as age, gender, BMI, the clinical characteristics and the metabolic parameters were compared between both groups. Among them, 184(22.9%) patients had been followed up for more than 24 months or they recurred during the follow up(mean: 56.0, median: 58.5, range: 7.0-140.0) and they were examined for the risk of stone recurrence by performing multivariate Cox regression analysis.
RESULTS
Obesity was significantly associated with the increased urinary excretion of sodium, calcium and oxalate(p<0.05, respectively). The urinary pH value showed inverse correlation with obesity(p=0.012). Urinary metabolic abnormalities were more common in the obese SF patients than the non-obese SF patients(p=0.003). Obesity was significantly associated with the stone recurrence rate(p=0.009). Cox regression analysis revealed that obesity was a strong predictor for recurrent stone formation(adjusted HR=2.384 95% CI: 1.372-4.143, p=0.002).
CONCLUSIONS
Our results reveal that obesity is highly associated with metabolic alterations and urinary stone recurrence. Therefore, weight control might be considered as one of the preventive measures against recurrent stone formation.
Keyword
MeSH Terms
Figure
-
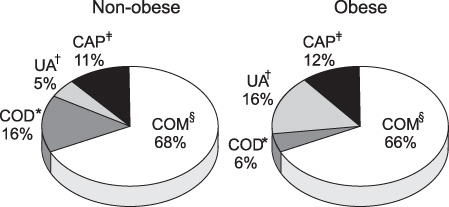
Fig. 1 Stone analysis with obesity (n=150). *COD: calcium oxalate dihydrate, †UA: uric acid, ‡CAP: calcium phosphate, §COM: calcium oxalate monohydrate.

Fig. 2 Rate of being stone recurrence free according to obesity (follow-up duration ≥2 years) (n=184).
Reference
-
1. Avogaro P, Crepaldi G, Enzi G, Tiengo A. Metabolic aspects of essential obesity. Epatologia. 1965. 11:226–238.2. DeFronzo RA, Ferrannini E. Insulin resistance. A multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Diabetes Care. 1991. 14:173–194.3. Gill T. Epidemiology and health impact of obesity: an Asian Pacific perspective. Asia Pac J Clin Nutr. 2006. 15:Suppl. 3–14.4. Taylor EN, Stampfer MJ, Curhan GC. Obesity, weight gain, and the risk of kidney stones. JAMA. 2005. 293:455–462.5. Nishio S, Yokoyama M, Iwata H, Takeuchi M, Kamei O, Sugamoto T. Obesity as one of the risk factors for urolithiasis. Nippon Hinyokika Gakkai Zasshi. 1998. 89:573–580.6. Powell CR, Stoller ML, Schwartz BF, Kane C, Gentle DL, Bruce JE, et al. Impact of body weight on urinary electrolytes in urinary stone formers. Urology. 2000. 55:825–830.7. Ekeruo WO, Tan YH, Young MD, Dahm P, Maloney ME, Mathias BJ, et al. Metabolic risk factors and the impact of medical therapy on the management of nephrolithiasis in obese patients. J Urol. 2004. 172:159–163.8. Siener R, Glatz S, Nicolay C, Hesse A. The role of overweight and obesity in calcium oxalate stone formation. Obes Res. 2004. 12:106–113.9. Curhan GC, Willett WC, Rimm EB, Speizer FE, Stampfer MJ. Body size and risk of kidney stones. J Am Soc Nephrol. 1998. 9:1645–1652.10. Deurenberg P, Yap M, van Staveren WA. Body mass index and percent body fat: a meta analysis among different ethnic groups. Int J Obes Relat Metab Disord. 1998. 22:1164–1171.11. WHO Expert Consultation. Appropriate body-mass index for asian populations and its implications for policy and intervention strategies. Lancet. 2004. 363:157–163.12. Lifshitz DA, Shalhav AL, Lingeman JE, Evan AP. Metabolic evaluation of stone disease patients: a practical approach. J Endourol. 1999. 13:669–678.13. Asper R. Epidemiology and socioeconomic aspects of urolithiasis. Urol Res. 1984. 12:1–5.14. Iguchi M, Umekawa T, Ishikawa Y, Katayama Y, Kodama M, Takada M, et al. Preparation of a standard diet for out-patients in the study of lithogenesis. Nippon Hinyokika Gakkai Zasshi. 1991. 82:378–387.15. Kim HJ, Jeon YS, Lee NK. Hyperlipidemia and obesity as a risk factor of urolithiasis. Korean J Urol. 2000. 41:763–766.16. Jo MK, Kwak C, Park SK, Yoo KY, Kang DH, Kim HH, et al. Prevalence and epidemiological characteristics of urolithiasis for adults aged 40-79 in Seoul, Korea. Korean J Urol. 2000. 41:367–374.17. Maalouf NM, Cameron MA, Moe OW, Sakkaee K. Novel insights into the pathogenesis of uric acid nephrolithiasis. Curr Opin Nephrol Hypertens. 2004. 13:181–189.18. Coe FL. Hyperuricosuric calcium oxalate nephrolithiasis. Adv Exp Med Biol. 1980. 128:439–450.19. Reddy ST, Wang CY, Sakhaee K, Brinkley L, Pak CY. Effect of low-carbohydrate high-protein diets on acid-base balance, stone-forming propensity, and calcium metabolism. Am J Kidney Dis. 2002. 40:265–274.20. Norman RW, Bath SS, Robertson WG, Peacock M. When should patients with symptomatic urinary stone disease be evaluated metabolically? J Urol. 1984. 132:1137–1139.21. Robertson WG. Medical management of urinary stone disease. Eur Urol Update Series. 1998. 7:139–144.22. Riccardi G, Giacco R, Rivellese AA. Dietary fat, insulin sensitivity and the metabolic syndrome. Clin Nutr. 2004. 23:447–456.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of obesity and metabolic health on urolithiasis: A nationwide population-based study
- Risk factors for urinary stone
- The Relationship between Obesity and the Risk Factors of Urolithiasis
- Efficacy of Standard Diet Therapy for Patients with Urolithiasis
- Comparison of Metabolic Risk Factors in Urolithiasis Patients according to Family History
