Paraplegia in a Patient With IgG4-Related Sclerosing Disease: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, Bundang Jesaeng Hospital, Seongnam, Korea. glide@dmc.or.kr
- 2Department of Neurosurgery, Bundang Jesaeng Hospital, Seongnam, Korea.
- 3Department of Pathology, Bundang Jesaeng Hospital, Seongnam, Korea.
- KMID: 2267099
- DOI: http://doi.org/10.5535/arm.2014.38.6.856
Abstract
- Immunoglobulin G4 (IgG4)-related sclerosing disease is a systemic disease, characterized by mass forming inflammatory lesions which respond well to steroid therapy. Pancreas is the most common site of involvement, and other organ involvements are also common. However, there are only a few reports about central nervous system involvement. We report a case of IgG4-related sclerosing disease which involves spinal cord causing paraplegia. A middle-aged female presented with sudden lower limb weakness. Magnetic resonance imaging showed a soft tissue mass which was diffusely compressing spinal cord along the C7 to T5 levels. Intravenous steroid pulse therapy and emergent operation was performed. The immunopathologic findings revealed IgG4-related sclerosing pachymeningitis postoperatively. There was no evidence of other organ involvement. Her neurologic deficit remained unchanged after two months of comprehensive rehabilitation therapy.
MeSH Terms
Figure
-

Fig. 1 Cervicothoracic magnetic resonance image shows tubular smooth-margined intradural extramedullary soft tissue mass from C7 to T5 levels with signal change on spinal cord. Sagittal T2-weighted (A) and gadoliniumenhanced T1-weighted (B) images. Axial T2-weighted (C) and gadolinium-enhanced T1-weighted (D) images.
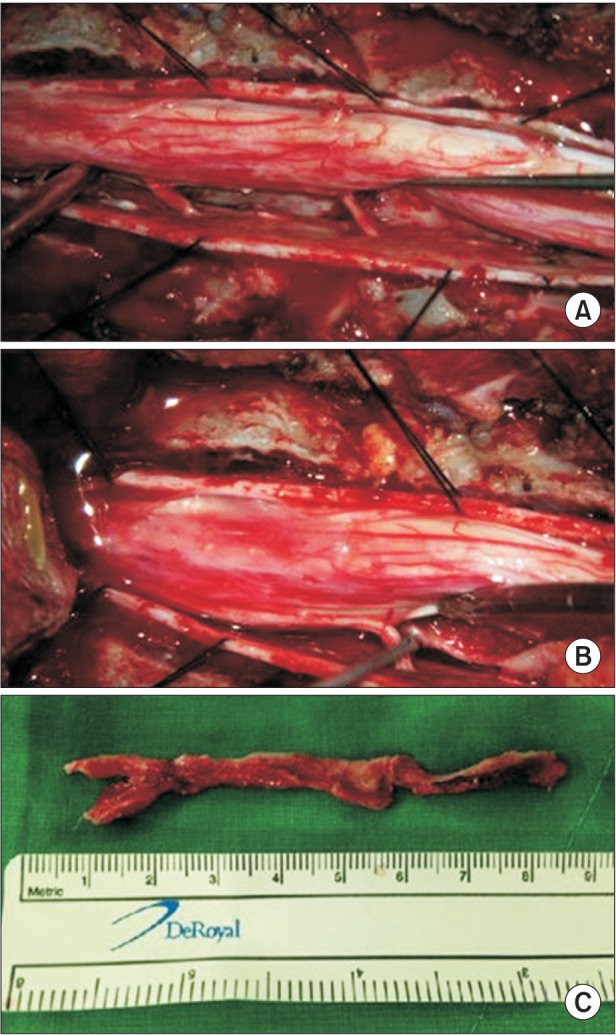
Fig. 2 Findings of intraoperative specimen. (A) Anterior located intradural extramedullary mass compressing the thoracic spinal cord. (B) Separation of the mass after sacrifice of the thoracic rootlets. (C) Whole mass after excision.
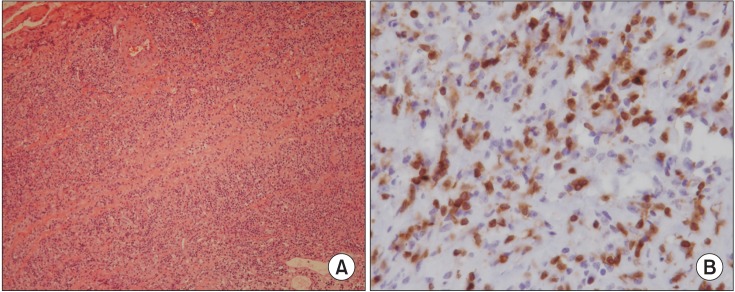
Fig. 3 Findings of microscopic examination. Dense lymphoid cell infiltration associated with fibrosis characterized by sclerotic collagen fibers. (A) The lymphoid cell infiltration consists of a mixture of mature plasma cells and small lymphocytes (H&E stain, ×100). (B) Immunostaining reveals IgG4 positive cells (×400).
Cited by 1 articles
-
A Case of IgG4 Related Pachymeningitis
Ji In Kim, Jin Taek Song, Hyeong Ju Kwon, Ji-Yong Lee
J Neurocrit Care. 2016;9(2):162-165. doi: 10.18700/jnc.160075.
Reference
-
1. Kamisawa T, Okamoto A. IgG4-related sclerosing disease. World J Gastroenterol. 2008; 14:3948–3955. PMID: 18609677.
Article2. Wallace ZS, Carruthers MN, Khosroshahi A, Carruthers R, Shinagare S, Stemmer-Rachamimov A, et al. IgG4-related disease and hypertrophic pachymeningitis. Medicine (Baltimore). 2013; 92:206–216. PMID: 23793110.
Article3. Lindstrom KM, Cousar JB, Lopes MB. IgG4-related meningeal disease: clinico-pathological features and proposal for diagnostic criteria. Acta Neuropathol. 2010; 120:765–776. PMID: 20844883.
Article4. Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001; 344:732–738. PMID: 11236777.
Article5. Saab ST, Hornick JL, Fletcher CD, Olson SJ, Coffin CM. IgG4 plasma cells in inflammatory myofibroblastic tumor: inflammatory marker or pathogenic link. Mod Pathol. 2011; 24:606–612. PMID: 21297584.
Article6. Ishihara M, Izumoto S, Iwatsuki K, Yoshimine T. Immunohistochemical study of multiple inflammatory pseudotumors with both brain and spinal cord involvement: case report. Neurol Med Chir (Tokyo). 2010; 50:246–250. PMID: 20339279.7. Chan SK, Cheuk W, Chan KT, Chan JK. IgG4-related sclerosing pachymeningitis: a previously unrecognized form of central nervous system involvement in IgG4-related sclerosing disease. Am J Surg Pathol. 2009; 33:1249–1252. PMID: 19561447.8. Choi SH, Lee SH, Khang SK, Jeon SR. IgG4-related sclerosing pachymeningitis causing spinal cord compression. Neurology. 2010; 75:1388–1390. PMID: 20938032.
Article9. Tajima Y, Mito Y. Cranial neuropathy because of IgG4-related pachymeningitis; intracranial and spinal mass lesions. BMJ Case Rep. 2012; 7. 19. [Epub]. http://dx.doi.org/10.1136/bcr-2012-006471.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of IgG4-Related Sclerosing Disease Involving the Eyelid in an Idiopathic Sclerosing Myositis Patient
- Immunoglobulin G4-related sclerosing cholangitis
- Advances in IgG4-related Hepatobiliary Disease
- A Case of Immunoglobulin G4-Related Sclerosing Disease Mimicking Lung Cancer
- A Case of Immunoglobulin G4-Related Sclerosing Disease not Responded to Steroid in Nasal Cavity
