A Case of Immunoglobulin G4-Related Sclerosing Disease not Responded to Steroid in Nasal Cavity
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, College of Medicine, Hanyang University, Seoul, Korea. ent@hanyang.ac.kr
- KMID: 2398834
- DOI: http://doi.org/10.18787/jr.2017.24.2.138
Abstract
- IgG4-related sclerosing disease was first discovered when researching autoimmune pancreatitis. It is an autoimmune disease that causes fibrosis on the pancreas, bile duct, gall bladder, salivary glands, and lungs. It is rarely reported in the nasal cavity. The diagnosis of IgG4-related sclerosing disease is based on biopsy findings demonstrating the characteristic histopathologic findings and immunohistochemical staining. IgG4-related sclerosing disease shows good response to high-dose steroid therapy. However, some patients do not respond to this treatment. Azathioprine or rituximab can be helpful in such case. We report our experience with IgG4-related sclerosing disease treated with azathioprine for 2 years, along with a related literature review.
MeSH Terms
Figure
-
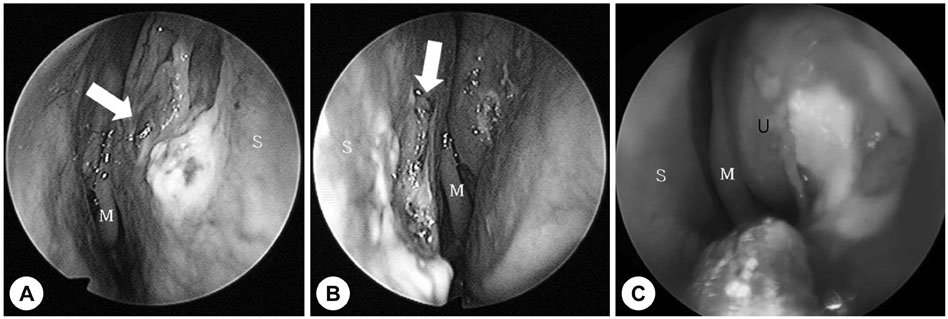
Fig. 1 Endoscopic findings of nasal cavity (2014.11.13). A: Large sized perforation (arrow) with very thin mucosal membrane and severe inflammation in right nasal cavity after crust removal. B: Left Nasal cavity before crust removal. White material is a Merocel packing to protect blood aspiration during deep biopsy. C: Ulcerative lesion (arrow) around left lateral nasal wall. U: Uncinate process, M: Middle turbinate, S: Septum.
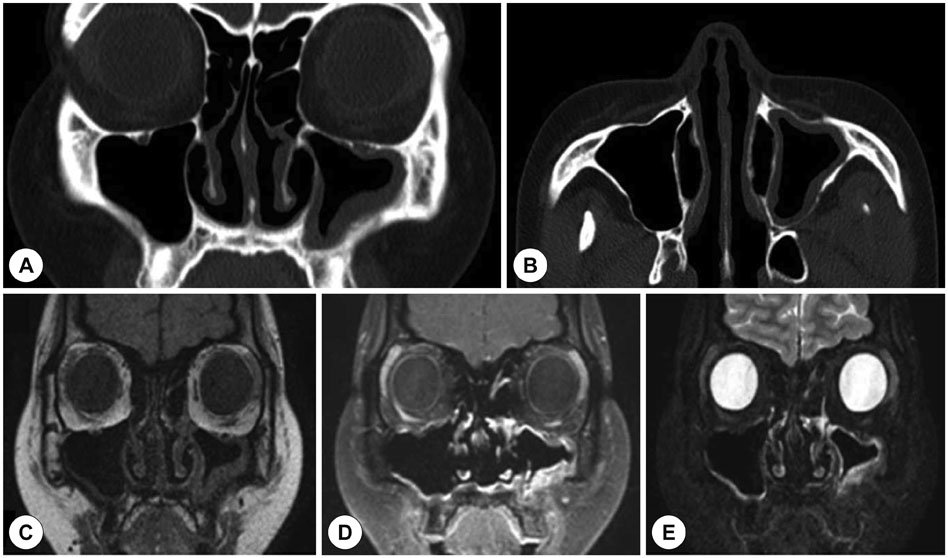
Fig. 2 Radiologic findings. CT image showing mucosal thickening of left maxillary sinus, Coronal view (A). Axial view (B). Coronal MR image showing mucosal thickening of supero-anterior portion of left lateral nasal wall with left maxillary mucosal thickening, T1-weighted image (C). T1-weighted with gadolinium enhancement (D). T2-weighted image (E).
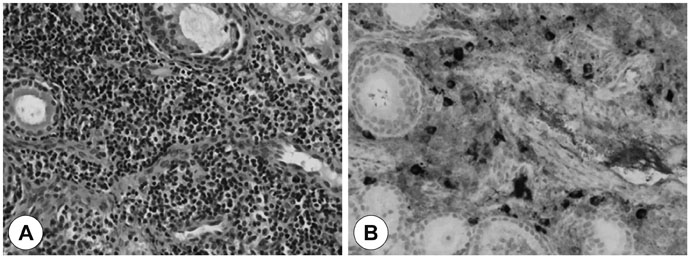
Fig. 3 Pathologic findings. It reveals fibrosclerotic change with marked lymphoplasmacytic inflammation (H&E, ×400) (A). It shows large Immunoglobulin G4 (IgG4)-positive plasma cell in fibrosclerotic stroma, measuring 35/HPF and the ratio of IgG4 with IgG is about 40% (IgG4 immunoperoxidase stain, ×400) (B).

Fig. 4 Endoscopic findings during treatment. Septal perforation with crust and ulcerative mucosal lesion was seen during treatment (After using azathioprine 1month, 14.3.31) (A). Well healed mucosa of nasal septum was seen after stop medication (16.2.14) (B).
Cited by 1 articles
-
A Case of IgG4-Related Disease With Sino-Nasal Involvement
Young Seok Han, Jun Sang Cha, Min Jung Jung, Joo Yeon Kim
Korean J Otorhinolaryngol-Head Neck Surg. 2022;65(11):705-712. doi: 10.3342/kjorl-hns.2021.00598.
Reference
-
1. Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012; 22(1):21–30.
Article2. Chen Y, Zhao JZ, Feng RE, Shi JH, Li XM, Fei YY, et al. Types of Organ Involvement in Patients with Immunoglobulin G4-related Disease. Chin Med J (Engl). 2016; 129(13):1525–1532.
Article3. Zen Y, Fujii T, Harada K, Kawano M, Yamada K, Takahira M, et al. Th2 and regulatory immune reactions are increased in immunoglobin G4-related sclerosing pancreatitis and cholangitis. Hepatology. 2007; 45(6):1538–1546.
Article4. Ishida M, Hotta M, Kushima R, Shibayama M, Shimizu T, Okabe H. Multiple IgG4-related sclerosing lesions in the maxillary sinus, parotid gland and nasal septum. Pathol Int. 2009; 59(9):670–675.
Article5. Sasaki T, Takahashi K, Mineta M, Fujita T, Aburano T. Immunoglobulin G4-Related Sclerosing Disease Mimicking Invasive Tumor in the Nasal Cavity and Paranasal Sinuses. AJNR Am J neuroradiol. 2012; 33(2):E19–E20.
Article6. Lee KK, Cho HP, Lee YM, Park JH. A case of immunoglobulin G4-related sialadenitis and dacryoadenitis. Korean J Otorhinolaryngol-Head Neck Surg. 2013; 56(7):444–447.
Article7. Yoon HJ, Park WS, Ji YB, Lee SH. Two Cases of Immunoglobulin G4-Related Sclerosing Disease Mimicking Nasopharyngeal Carcinoma. Korean J Otorhinolaryngol-Head Neck Surg. 2016; 59(4):304–308.
Article8. Suzuki M, Nakamaru Y, Akazawa S, Mizumachi T, Maeda M, Takagi D, et al. Nasal manifestations of immunoglobulin G4-related disease. Laryngoscope. 2013; 123(4):829–834.
Article9. Okazaki K, Uchida K, Miyoshi H, Ikeura T, Takaoka M, Nishio A. Recent concepts of autoimmune pancreatitis and IgG4-related disease. Clin Rev Allergy Immunol. 2011; 41(2):126–138.
Article10. Ikeda R, Awataguchi T, Shoji F, Oshima T. A case of paranasal sinus lesions in IgG4-related sclerosing disease. Otolaryngol Head Neck Surg. 2010; 142(3):458–459.
Article11. Pace C, Ward S. A rare case of IgG4-related sclerosing disease of the maxillary sinus associated with bone destruction. J Oral Maxillofac Surg. 2010; 68(10):2591–2593.
Article12. Lee JR, Lee BJ, Chung YS. Three Cases of IgG4-Related Sclerosing Disease in Nasal Cavity. J Rhinol. 2016; 23(1):44–48.
Article13. Kitagawa S, Zen Y, Harada K, Sasaki M, Sato Y, Minato H, et al. Abundant IgG4-positive plasma cell infiltration characterizes chronic sclerosing sialadenitis (Küttner's tumor). Am J Surg Pathol. 2005; 29(6):783–791.
Article14. Masaki Y, Kurose N, Umehara H. IgG4-related disease: a novel lymphoproliferative disorder discovered and established in Japan in the 21st century. J Clin Exp Hematop. 2011; 51(1):13–20.
Article15. Lindau RH, Su YB, Kobayashi R, Smith RB. Immunoglobulin G4-related sclerosing disease of the paranasal sinus. Head Neck. 2013; 35(10):E321–E324.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immunoglobulin G4-related sclerosing cholangitis
- A Case of Immunoglobulin G4-Related Sclerosing Disease Mimicking Lung Cancer
- Immunoglobulin G4-Related Systemic Sclerosing Disease: A Case Involving the Ureter and Kidney
- A 2-Week Steroid Trial for Differentiating Isolated IgG4-Related Sclerosing Cholangitis from Cholangiocarcinoma
- Two Cases of Immunoglobulin G4-Related Sclerosing Disease Mimicking Nasopharyngeal Carcinoma
