Pharmacokinetics of T-614 after Single Oral Administration in Healthy Korean Volunteers
- Affiliations
-
- 1Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital, Korea. ksyu@snu.ac.kr
- 2Department of Clinical Pharmacology and Therapeutics, Kyung Hee University Hospital, Korea.
- 3Department of Clinical Pharmacology and Therapeutics, Samsung Medical Center, Korea.
- KMID: 2203228
- DOI: http://doi.org/10.12793/jkscpt.2013.21.2.150
Abstract
- BACKGROUND
Iguratimod is a new type of disease modifying anti-rheumatic drug, which reduced the production of inflammatory cytokines. The purpose of this study was to evaluate pharmacokinetic characteristics and safety profiles of iguratimod after a single oral administration in healthy Korean volunteers.
METHODS
A randomized, double-blind, placebo-controlled, parallel group, single oral dose study was conducted in 24 healthy male volunteers. Three groups of eight subjects each received 25 mg, 50 mg, or 100 mg dosage, respectively. Two subjects in each dose group were administered matching placebo. Plasma concentrations of iguratimod were measured till 72 hours after drug administration. Tolerability was evaluated by monitoring adverse events, clinical laboratory tests, and 12-lead electrocardiograms.
RESULTS
The mean area under the concentration-time curve from 0 to 72 hours (AUClast) were 11.9, 25.2, and 51.8 mg x h/L and the maximum plasma concentration (Cmax) were 1.15, 2.33, and 4.78 mg/L in 25, 50 and 100 mg dose groups, respectively. All doses of iguratimod were well tolerated without serious adverse events or clinically meaningful changes.
CONCLUSION
Cmax and AUClast values of iguratimod proportionally increased with incremental dose. Iguratimod was generally safe and well tolerated.
Keyword
MeSH Terms
Figure
-
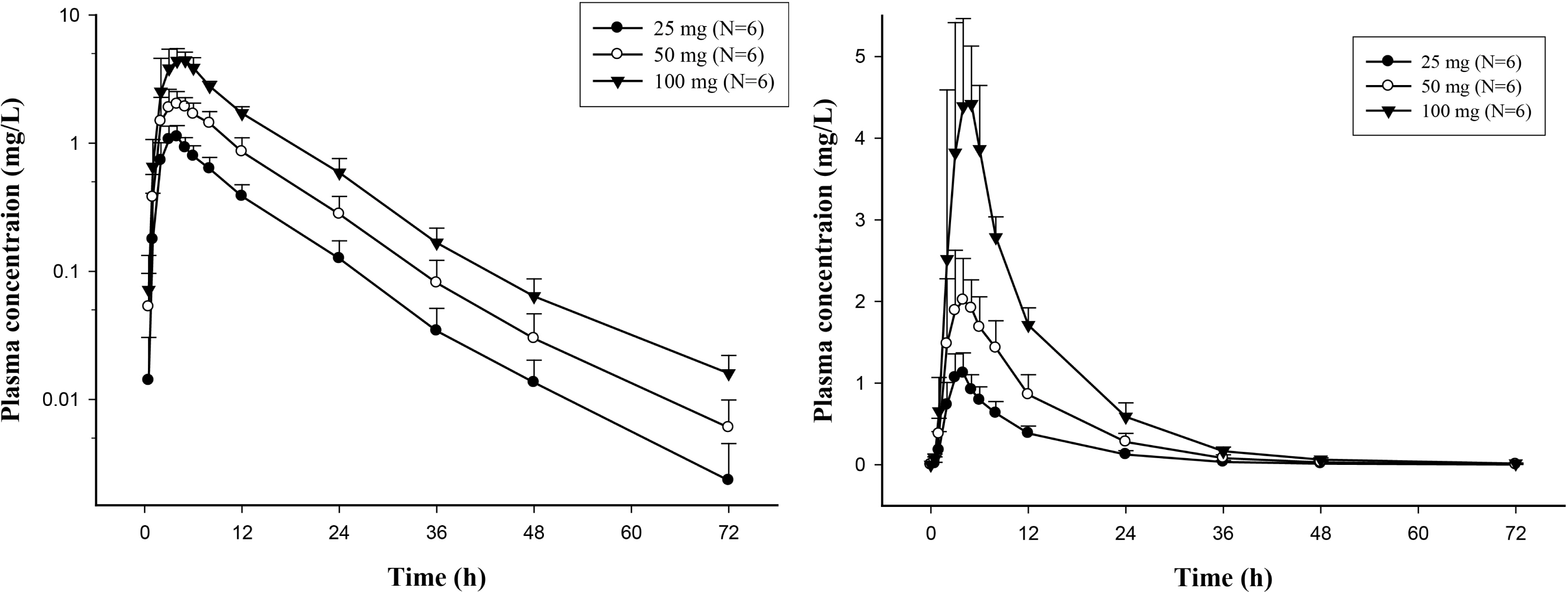
Figure 1. Mean plasma concentration-time profiles after oral administration of Iguratimod 25, 50 and 100 mg in healthy Korean subjects. Left panel, semi-log scale; right panel linear scale. Bars represent standard deviations.
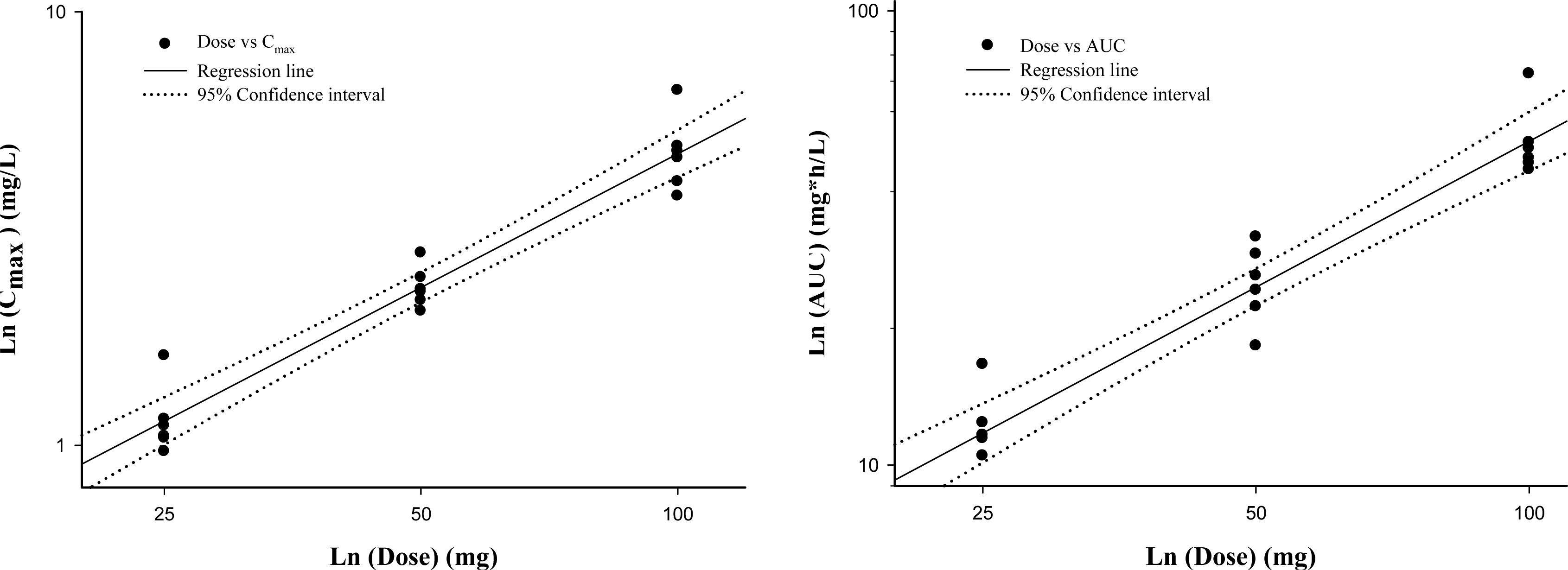
Figure 2. Relationship between pharmacokinetic parameters and dose following single oral Iguratimod doses of 25, 50 and 100 mg. Left panel, log-transformed Cmax-dose relationship and right panel, log-transformed AUClast-dose relationship of Iguratimod.
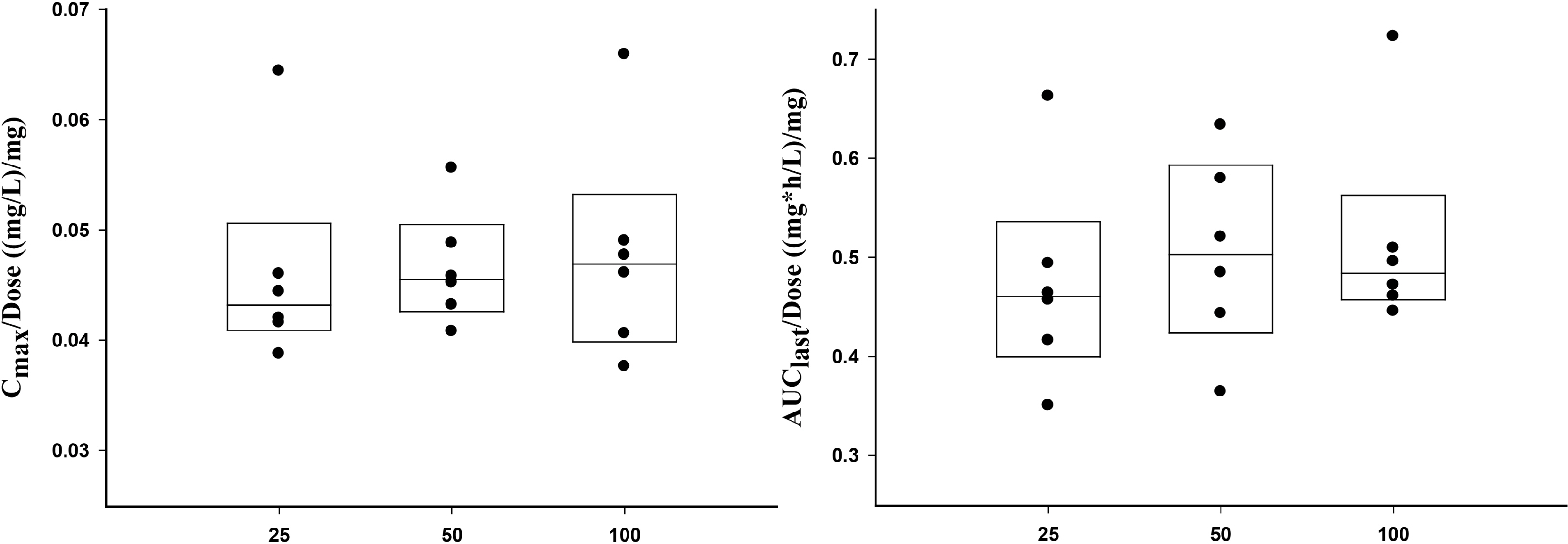
Figure 3. Comparison of dose-normalized Cmax and AUClast after single oral administration of Iguratimod 25, 50 and 100 mg. The box edges show lower (25 th) and upper (75 th) quartiles and the line in the middle indicates the median value. Left panel, dose-normalized Cmax and right panel, dose-normalized AUClast.
Reference
-
1. Koch AE. Review: angiogenesis: implications for rheumatoid arthritis. Arthritis Rheum. 1998; 41(6):951–962.2. Walsh DA. Angiogenesis and arthritis. Rheumatology (Oxford). 1999; 38(2):103–112.
Article3. Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010; 376(9746):1094–1108.
Article4. Sawada T, Hashimoto S, Tohma S, Nishioka Y, Nagai T, Sato T, Ito K, Inoue T, Iwata M, Yamamoto K. Inhibition of L-leucine methyl ester mediated killing of THP-1, a human monocytic cell line, by a new anti-inflammatory drug, T614. Immunopharmacology. 2000; 49(3):285–294.
Article5. Tanaka K, Kawasaki H, Kurata K, Aikawa Y, Tsukamoto Y, Inaba T. Iguratimod, a novel antirheumatic drug, inhibits both the activity and induction of cyclooxygenase-2 (COX-2) in cultured fibroblasts. Jpn J Pharmacol. 1995; 67(4):305–314.6. Scrivo R, Di Franco M, Spadaro A, Valesini G. The immunology of rheumatoid arthritis. Ann N Y Acad Sci. 2007; 1108:312–322.
Article7. van der Linden MP, van der Woude D, Ioan-Facsinay A, Levarht EW, Stoeken-Rijsbergen G, Huizinga TW, Toes RE & van der Helm-van Mil AH. Value of anti-modified citrullinated vimentin and third-generation anti-cyclic citrullinated peptide compared with second-generation anti-cyclic citrullinated peptide and rheumatoid factor in predicting disease outcome in undifferentiated arthritis and rheumatoid arthritis. Arthritis Rheum. 2009; 60(8):2232–2241.
Article8. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis Rheum. 2002; 46(2):328–346.9. Smolen JS, Landewe R, Breedveld FC, Dougados M, Emery P, Gaujoux-Viala C, Gorter S, Knevel R, Nam J, Schoels M, Aletaha D, Buch M, Gossec L, Huizinga T, Bijlsma JW, Burmester G, Combe B, Cutolo M, Gabay C, Gomez-Reino J, Kouloumas M, Kvien TK, Martin-Mola E, McInnes I, Pavelka K, van Riel P, Scholte M, Scott DL, Sokka T, Valesini G, van Vollenhoven R, Winthrop KL, Wong J, Zink A, van der Heijde D. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs. Ann Rheum Dis. 2010; 69(6):964–975.
Article10. Carmona L, Cross M, Williams B, Lassere M, March L. Rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2010; 24(6):733–745.
Article11. Smolen JS, Aletaha D, Koeller M, Weisman MH, Emery P. New therapies for treatment of rheumatoid arthritis. Lancet. 2007; 370(9602):1861–1874.
Article12. Kawakami A, Tsuboi M, Urayama S, Matsuoka N, Yamasaki S, Hida A, Aoyagi T, Furuichi I, Nakashima T, Migita K, Kawabe Y, Nakashima M, Origuchi T, Eguchi K. Inhibitory effect of a new anti-rheumatic drug Iguratimod on costimulatory molecule expression, cytokine production, and antigen presentation by synovial cells. J Lab Clin Med. 1999; 133(6):566–574.13. Kuriyama K, Higuchi C, Tanaka K, Yoshikawa H, Itoh K. A novel anti-rheumatic drug, Iguratimod, stimulates osteoblastic differentiation in vitro and bone morphogenetic protein-2-induced bone formation in vivo. Biochem Biophys Res ommun. 2002; 299(5):903–909.14. Lu LJ, Bao CD, Dai M, Teng JL, Fan W, Du F, Yang NP, Zhao YH, Chen ZW, Xu JH, He PG, Wu HX, Tao Y, Zhang MJ, Han XH, Li XF, Gu JR, Li JH, Yu H. Multicenter, randomized, double-blind, controlled trial of treatment of active rheumatoid arthritis with Iguratimod compared with methotrexate. Arthritis Rheum. 2009; 61(7):979–987.15. Hara M, Abe T, Sugawara S, Mizushima Y, Hoshi K, Irimajiri S, Hashimoto H, Yoshino S, Matsui N, Nobunaga M. Long-term safety study of Iguratimod in patients with rheumatoid arthritis. Mod Rheumatol. 2007; 17(1):10–16.
Article16. Hara M, Abe T, Sugawara S, Mizushima Y, Hoshi K, Irimajiri S, Hashimoto H, Yoshino S, Matsui N, Nobunaga M, Nakano S. Efficacy and safety of Iguratimod compared with placebo and salazosulfapyridine in active rheumatoid arthritis: a controlled, multicenter, double-blind, parallel-group study. Mod Rheumatol. 2007; 17(1):1–9.
Article17. Nakashima K, Zhou X, Kunkel G, Zhang Z, Deng JM, Behringer RR, de Crombrugghe B. The novel zinc finger-containing transcription factor osterix is required for osteoblast differentiation and bone formation. Cell. 2002; 108(1):17–29.
Article18. Tanaka K, Urata N, Mikami M, Ogasawara M, Matsunaga T, Terashima N, Suzuki H. Effect of Iguratimod and other anti-rheumatic drugs on adenocarcinoma colon 26-induced cachexia in mice. Inflamm Res. 2007; 56(1):17–23.
Article19. Lu LJ, Teng JL, Bao CD, Han XH, Sun LY, Xu JH, Li XF, Wu HX. Safety and efficacy of Iguratimod in the treatment of patients with active rheumatoid arthritis: a double blind, randomized, placebo-controlled and multicenter trial. Chin Med J (Engl). 2008; 121(7):615–619.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Population pharmacokinetics and inter-laboratory variability of sildenafil and its metabolite after oral administration in Korean healthy male volunteers
- Pharmacokinetics and Safety of Duloxetine Enteric-coated Tablets in Chinese Healthy Volunteers: A Randomized, Open-label, Single- and Multiple-dose Study
- Tolerability and Pharmacokinetics Following a Single Dose of Vardenafil in Healthy Korean Volunteers
- Pharmacokinetic Characteristics of Cefcapene Pivoxil Hydrochloride after Single Oral Administration in Healthy Korean Subjects
- Comparative pharmacokinetics between tenofovir disoproxil phosphate and tenofovir disoproxil fumarate in healthy subjects
