Clinical Utility of Coronary CT Angiography with Stress Perfusion CT in Preoperative Cardiac Risk Evaluation
- Affiliations
-
- 1Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. dkkim@skku.edu
- 2Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Vascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Cardiovascular Imaging Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2145478
- DOI: http://doi.org/10.4070/kcj.2014.44.3.170
Abstract
- BACKGROUND AND OBJECTIVES
Vascular surgery carries high operative risk. Recently developed cardiac computed tomography (CT) provides excellent imaging of coronary artery disease (CAD), as well as myocardial perfusions. We investigated the role of stress perfusion CT with coronary computed tomography angiography (CCTA) using 128-slice dual source CT (DSCT) in preoperative cardiac risk evaluation.
SUBJECTS AND METHODS
Patients scheduled for vascular surgery were admitted and underwent the adenosine stress perfusion CT with CCTA using DSCT. Patients who presented with unstable angina, recent myocardial infarction, decompensated heart failure, or renal failure were excluded. Stress perfusion CT was first acquired using sequential mode during adenosine infusion, after which, scanning for CT angiography was followed by helical mode. Perioperative events were followed up for 1 month.
RESULTS
Ninety-one patients completed the study. Most patients (94.5%) had coronary atherosclerosis, with 36 (39.6%) patients had more than 50% coronary artery stenosis. Perfusion defects with significant stenosis were found in 12 cases (13.2%). Revascularization after DSCT was rarely performed. Four patients (4.4%) experienced cardiac events in the perioperative period: two experienced heart failure and two had non-fatal myocardial infarction.
CONCLUSION
We cannot conclude that the stress perfusion CT, with CCTA using DSCT, plays a significant role in preoperative risk evaluation from this study. However, the coronary atherosclerosis and the significant CAD were commonly found. The perfusion defects with significant lesions were found in only small fraction of the patients, and did not contribute to perioperative myocardial infarction or heart failure.
Keyword
MeSH Terms
Figure
-
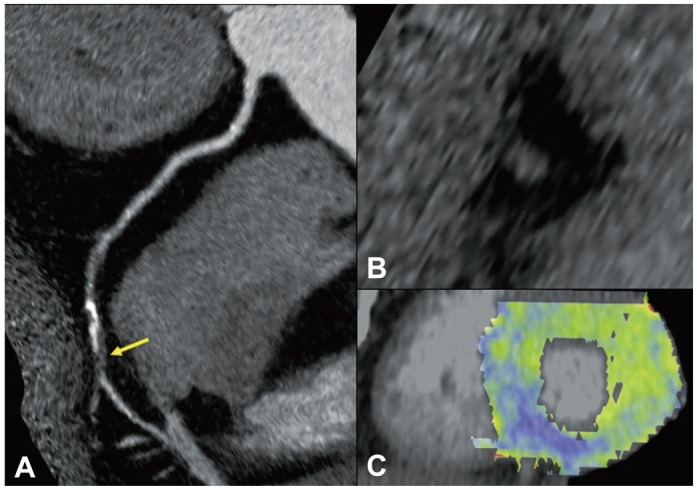
Fig. 1 Analysis of CTA and stress perfusion CT image. Patients with significant stenosis with stress induced perfusion defect in RCA territory. CTA shows tight stenosis in mid RCA (A and B), and the corresponding myocardial segments in basal inferior wall shows significant perfusion defect in stress perfusion CT image (C). CTA: computed tomographic angiography, CT: computed tomography, RCA: right coronary artery.
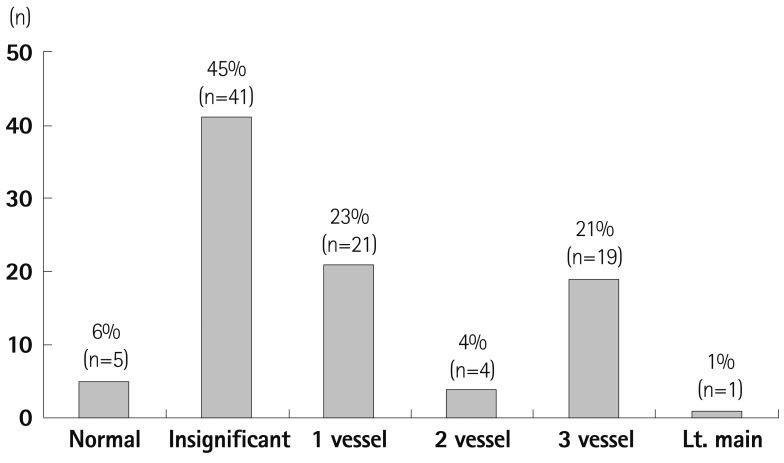
Fig. 2 Extent of coronary artery disease: CCTA results. Multivessel disease (24%) was prevalent in the patients who underwent vascular surgery. Coronary atherosclerosis was found in most of the patients (94%) (History of coronary revascularization and insignificant stenosis in current CCTA has been considered as significantly diseased vessel in this analysis). CCTA: coronary computed tomography angiography.
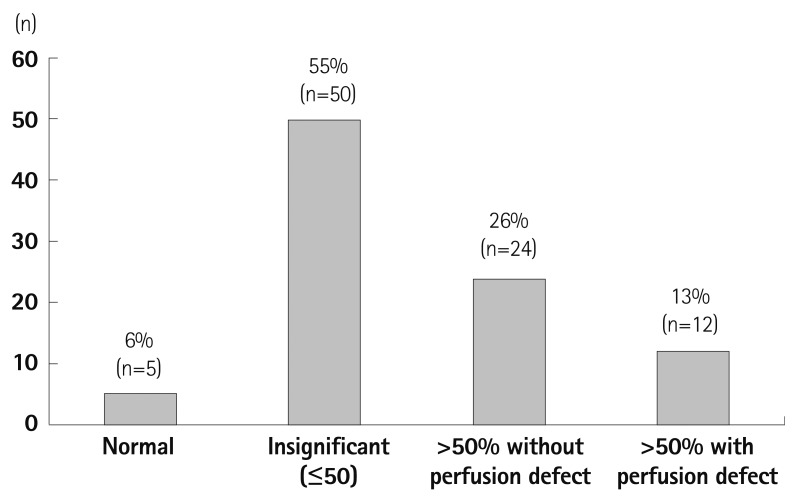
Fig. 3 Result of CCTA and perfusion CT. 94% of the patients had plaques in their coronary arteries and 39% had coronary artery stenosis of more than 50%. However, only a third of the patients with CAD (>50% stenosis) showed a perfusion defect (History of coronary revascularization and insignificant stenosis in current CTA has been considered "insignificant" in this analysis). CCTA: coronary computed tomography angiography, CT: computed tomography, CAD: coronary artery disease.
Reference
-
1. Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery--executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1996 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). J Am Coll Cardiol. 2002; 39:542–553. PMID: 11823097.2. Hamon M, Biondi-Zoccai GG, Malagutti P, et al. Diagnostic performance of multislice spiral computed tomography of coronary arteries as compared with conventional invasive coronary angiography: a meta-analysis. J Am Coll Cardiol. 2006; 48:1896–1910. PMID: 17084268.3. Feuchtner G, Goetti R, Plass A, et al. Adenosine stress high-pitch 128-slice dual-source myocardial computed tomography perfusion for imaging of reversible myocardial ischemia: comparison with magnetic resonance imaging. Circ Cardiovasc Imaging. 2011; 4:540–549. PMID: 21862731.4. Kim SM, Kim YN, Choe YH. Adenosine-stress dynamic myocardial perfusion imaging using 128-slice dual-source CT: optimization of the CT protocol to reduce the radiation dose. Int J Cardiovasc Imaging. 2013; 29:875–884. PMID: 23076604.5. Abbara S, Arbab-Zadeh A, Callister TQ, et al. SCCT guidelines for performance of coronary computed tomographic angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2009; 3:190–204. PMID: 19409872.6. Chang SA, Choi SI, Choi EK, et al. Usefulness of 64-slice multidetector computed tomography as an initial diagnostic approach in patients with acute chest pain. Am Heart J. 2008; 156:375–383. PMID: 18657674.7. Mahnken AH, Klotz E, Pietsch H, et al. Quantitative whole heart stress perfusion CT imaging as noninvasive assessment of hemodynamics in coronary artery stenosis: preliminary animal experience. Invest Radiol. 2010; 45:298–305. PMID: 20421799.8. Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Int J Cardiovasc Imaging. 2002; 18:539–542. PMID: 12135124.9. Einstein AJ, Moser KW, Thompson RC, Cerqueira MD, Henzlova MJ. Radiation dose to patients from cardiac diagnostic imaging. Circulation. 2007; 116:1290–1305. PMID: 17846343.10. Hertzer NR, Beven EG, Young JR, et al. Coronary artery disease in peripheral vascular patients. A classification of 1000 coronary angiograms and results of surgical management. Ann Surg. 1984; 199:223–233. PMID: 6696538.11. Baron JF, Mundler O, Bertrand M, et al. Dipyridamole-thallium scintigraphy and gated radionuclide angiography to assess cardiac risk before abdominal aortic surgery. N Engl J Med. 1994; 330:663–669. PMID: 8107716.12. Seki M, Kashimoto S, Nagata O, et al. Are the incidences of cardiac events during noncardiac surgery in Japan the same as in the United States and Europe? Anesth Analg. 2005; 100:1236–1240. PMID: 15845660.13. de Virgilio C, Bui H, Donayre C, et al. Endovascular vs open abdominal aortic aneurysm repair: a comparison of cardiac morbidity and mortality. Arch Surg. 1999; 134:947–950. discussion 950-1. PMID: 10487588.14. De Bruin JL, Baas AF, Buth J, et al. Long-term outcome of open or endovascular repair of abdominal aortic aneurysm. N Engl J Med. 2010; 362:1881–1889. PMID: 20484396.15. Boucher CA, Brewster DC, Darling RC, Okada RD, Strauss HW, Pohost GM. Determination of cardiac risk by dipyridamole-thallium imaging before peripheral vascular surgery. N Engl J Med. 1985; 312:389–394. PMID: 3871502.16. Poldermans D, Fioretti PM, Forster T, et al. Dobutamine stress echocardiography for assessment of perioperative cardiac risk in patients undergoing major vascular surgery. Circulation. 1993; 87:1506–1512. PMID: 8491005.17. Mason JJ, Owens DK, Harris RA, Cooke JP, Hlatky MA. The role of coronary angiography and coronary revascularization before noncardiac vascular surgery. JAMA. 1995; 273:1919–1925. PMID: 7783301.18. McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med. 2004; 351:2795–2804. PMID: 15625331.19. Russo V, Gostoli V, Lovato L, et al. Clinical value of multidetector CT coronary angiography as a preoperative screening test before noncoronary cardiac surgery. Heart. 2007; 93:1591–1598. PMID: 17164488.20. Budde RP, Huo F, Cramer MJ, et al. Simultaneous aortic and coronary assessment in abdominal aortic aneurysm patients by thoraco-abdominal 64-detector-row CT angiography: estimate of the impact on preoperative management: a pilot study. Eur J Vasc Endovasc Surg. 2010; 40:196–201. PMID: 20427209.21. Catalán P, Leta R, Hidalgo A, et al. Ruling out coronary artery disease with noninvasive coronary multidetector CT angiography before noncoronary cardiovascular surgery. Radiology. 2011; 258:426–434. PMID: 21079198.22. Kim SM, Chang SA, Shin W, Choe YH. Dual-energy CT perfusion during pharmacologic stress for the assessment of myocardial perfusion defects using a second-generation dual-source CT: a comparison with cardiac magnetic resonance imaging. J Comput Assist Tomogr. 2014; 38:44–52. PMID: 24424556.23. Kurata A, Kawaguchi N, Kido T, et al. Qualitative and quantitative assessment of adenosine triphosphate stress whole-heart dynamic myocardial perfusion imaging using 256-slice computed tomography. PLoS One. 2013; 8:e83950. PMID: 24376774.24. Blankstein R, Shturman LD, Rogers IS, et al. Adenosine-induced stress myocardial perfusion imaging using dual-source cardiac computed tomography. J Am Coll Cardiol. 2009; 54:1072–1084. PMID: 19744616.25. Rocha-Filho JA, Blankstein R, Shturman LD, et al. Incremental value of adenosine-induced stress myocardial perfusion imaging with dual-source CT at cardiac CT angiography. Radiology. 2010; 254:410–419. PMID: 20093513.
