Korean Circ J.
2010 Oct;40(10):514-519. 10.4070/kcj.2010.40.10.514.
Beneficial Effect of Efonidipine, an L- and T-Type Dual Calcium Channel Blocker, on Heart Rate and Blood Pressure in Patients With Mild-to-Moderate Essential Hypertension
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Bundang Hospital, Seongnam, Korea. cheolkim@plaza.snu.ac.kr
- 2Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Internal Medicine, Hanyang University College of Medicine, Guri Hospital, Guri, Korea.
- 4Department of Internal Medicine, Daegu Catholic University College of Medicine, Daegu, Korea.
- 5Department of Internal Medicine, Chonbuk National University College of Medicine, Jeonju, Korea.
- 6Department of Internal Medicine, Soonchunhyang University College of Medicine, Seoul, Korea.
- 7Department of Internal Medicine, Hallym University College of Medicine, Seoul, Korea.
- 8Department of Internal Medicine, Yonsei University College of Medicine, Gangnam Severance Hospital, Seoul, Korea.
- KMID: 1826140
- DOI: http://doi.org/10.4070/kcj.2010.40.10.514
Abstract
- BACKGROUND AND OBJECTIVES
Efonidipine hydrochloride, an L- and T-type dual calcium channel blocker, is suggested to have a heart rate (HR)-slowing action in addition to a blood pressure (BP)-lowering effect. The aim of this study was to determine the effect of efonidipine on HR and BP in patients with mild-to-moderate hypertension.
SUBJECTS AND METHODS
In a multi-center, prospective, open-labeled, single-armed study, we enrolled 53 patients who had mild-to-moderate hypertension {sitting diastolic BP (SiDBP) 90-110 mmHg}. After a 2-week washout, eligible patients were treated with efonidipine (40 mg once daily for 12 weeks). The primary end point was the change in HR from baseline to week 12. The secondary end-point included the change in trough sitting BP and 24-hour mean BP between baseline and week 12. Laboratory and clinical adverse events were monitored at each study visit (4, 8, and 12 weeks).
RESULTS
Fifty-two patients were included in the intention-to-treat analysis. After 12 weeks of treatment with efonidipine, the resting HR decreased significantly from baseline to week 12 {from 81.5+/-5.3 to 71.8+/-9.9 beats/minute (difference, -9.9+/-9.0 beats/minute), p<0.0001}. The trough BP {sitting systolic blood pressure (SiSBP) and SiDBP} and 24-hour mean BP also decreased significantly (SiSBP: from 144.6+/-8.2 to 132.9+/-13.5 mmHg, p<0.0001; SiDBP: from 96.9+/-5.4 to 88.3+/-8.6 mmHg, p<0.0001, 24-hour mean systolic BP: from 140.4+/-13.5 to 133.8+/-11.6 mmHg, p<0.0001; 24-hour mean diastolic BP: from 91.7+/-8.7 to 87.5+/-9.5 mmHg, p<0.0001).
CONCLUSION
Efonidipine was effective in controlling both HR and BP in patients with mild-to-moderate hypertension.
Keyword
MeSH Terms
Figure
-
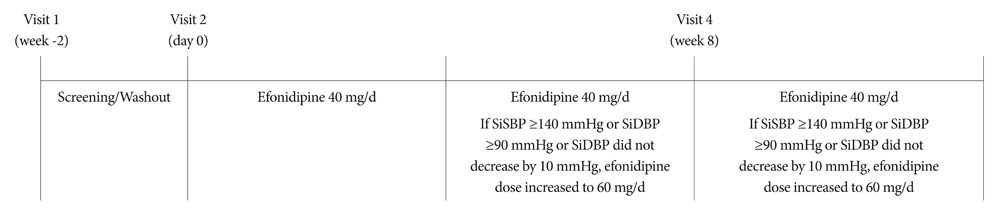
Fig. 1 Study design. SiSBP: sitting systolic blood pressure, SiDBP: sitting diastolic blood pressure.
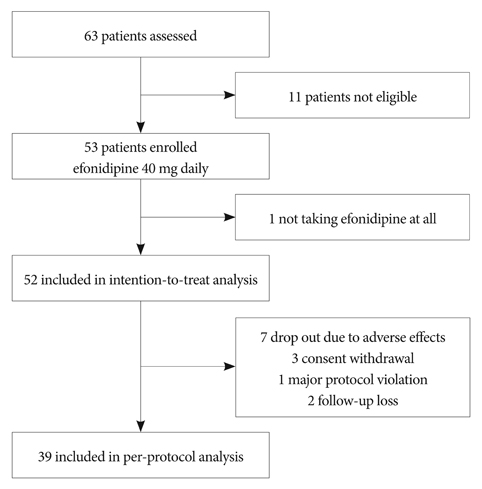
Fig. 2 Disposition of study patients.
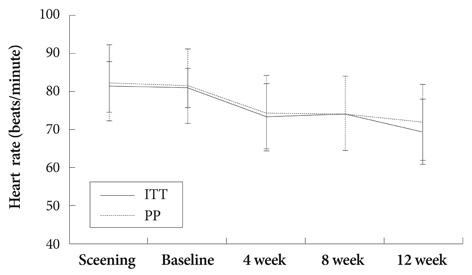
Fig. 3 Effects of efonidipine on heart rate at 4, 8, and 12 weeks. The reduction in heart rate was maintained during the active treatment period. ITT: intention-to-treat, PP: per-protocol.
Reference
-
1. Tanaka H, Shigenobu K. Efonidipine hydrochloride: a dual blocker of L- and T-type ca(2+) channels. Cardiovasc Drug Rev. 2002. 20:81–92.2. Hagiwara N, Irisawa H, Kameyama M. Contribution of two types of calcium currents to the pacemaker potentials of rabbit sino-atrial node cells. J Physiol. 1988. 395:233–253.3. Masumiya H, Shijuku T, Tanaka H, Shigenobu K. Inhibition of myocardial L- and T-type Ca2+ currents by efonidipine: possible mechanism for its chronotropic effect. Eur J Pharmacol. 1998. 349:351–357.4. Tanaka T, Tsutamoto T, Sakai H, Fujii M, Yamamoto T, Horie M. Comparison of the effects of efonidipine and amlodipine on aldosterone in patients with hypertension. Hypertens Res. 2007. 30:691–697.5. Shimizu M, Ogawa K, Sasaki H, et al. Effects of efonidipine, an L- and T-Type dual calcium channel blocker, on heart rate and blood pressure in patients with mild to severe hypertension: an uncontrolled, open-label pilot study. Curr Ther Res. 2003. 64:707–714.6. Diaz A, Bourassa MG, Guertin MC, Tardif JC. Long-term prognostic value of resting heart rate in patients with suspected or proven coronary artery disease. Eur Heart J. 2005. 26:967–974.7. Jouven X, Empana JP, Schwartz PJ, Desnos M, Courbon D, Ducimetiere P. Heart-rate profile during exercise as a predictor of sudden death. N Engl J Med. 2005. 352:1951–1958.8. Palatini P, Benetos A, Grassi G, et al. Identification and management of the hypertensive patient with elevated heart rate: statement of a European Society of Hypertension Consensus Meeting. J Hypertens. 2006. 24:603–610.9. Gillman MW, Kannel WB, Belanger A, D'Agostino RB. Influence of heart rate on mortality among persons with hypertension: the Framingham Study. Am Heart J. 1993. 125:1148–1154.10. Chung JW, Lee HY, Kim CH, et al. Losartan/hydrochlorothiazide fixed combination versus amlodipine monotherapy in Korean patients with mild to moderate hypertension. Korean Circ J. 2009. 39:151–156.11. Fox K, Borer JS, Camm AJ, et al. Resting heart rate in cardiovascular disease. J Am Coll Cardiol. 2007. 50:823–830.12. Cha DH, Cha YS, Kook JH, et al. Clinical efficacy of carvedilol in patients with moderate to severe congestive heart failure. Korean Circ J. 1998. 28:523–531.13. The Israeli Sprint Study Group. Secondary prevention reinfarction Israeli nifedipine trial (SPRINT): a randomized intervention trial of nifedipine in patients with acute myocardial infarction. Eur Heart J. 1988. 9:354–364.14. Goldbourt U, Behar S, Reicher-Reiss H, Zion M, Mandelzweig L, Kaplinsky E. Early administration of nifedipine in suspected acute myocardial infarction. The Secondary Prevention Reinfarction Israel Nifedipine Trial 2 Study. Arch Intern Med. 1993. 153:345–353.15. Furberg CD, Psaty BM, Meyer JV. Nifedipine: Dose-related increase in mortality in patients with coronary heart disease. Circulation. 1995. 92:1326–1331.16. Psaty BM, Heckbert SR, Koepsell TD, et al. The risk of myocardial infarction associated with antihypertensive drug therapies. JAMA. 1995. 274:620–625.17. Kim DW, Seo JD, Cho SW, et al. Antihypertensive efficacy and safety of perindopril versus nifedipine in high salt intake essential hypertensives: a double-blind parallel group study. Korean Circ J. 1994. 24:156–163.18. Furukawa T, Nukada T, Miura R, et al. Differential blocking action of dihydropyridine Ca2+ antagonists on a T-type Ca2+ channel (alpha1G) expressed in Xenopus oocytes. J Cardiovasc Pharmacol. 2005. 45:241–246.19. Furukawa T, Yamakawa T, Midera T, Sagawa T, Mori Y, Nukada T. Selectivities of dihydropyridine derivatives in blocking Ca(2+) channel subtypes expressed in Xenopus oocytes. J Pharmacol Exp Ther. 1999. 291:464–473.20. Morimoto S, Jo F, Maki K, Iwasaka T. Effects of efonidipine hydrochloride on heart rate and circulatory changes due to stress. Clin Exp Hypertens. 2009. 31:83–91.21. Kinoshita H, Kuwahara K, Takano M, et al. T-type Ca2+ channel blockade prevents sudden death in mice with heart failure. Circulation. 2009. 120:743–752.22. Bloch MJ. British hypertension society recommends that beta-blockers are no longer indicated as initial treatment of hypertension: has the pendulum swung too far? J Clin Hypertens (Greenwich). 2007. 9:99–102.23. Lindholm LH, Carlberg B, Samuelsson O. Should beta blockers remain first choice in the treatment of primary hypertension: a meta-analysis. Lancet. 2005. 366:1545–1553.24. Palatini P, Benetos A, Julius S. Impact of increased heart rate on clinical outcomes in hypertension: implications for antihypertensive drug therapy. Drugs. 2006. 66:133–144.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of an L- and T-Type Calcium Channel Blocker on 24-Hour Systolic Blood Pressure and Heart Rate in Hypertensive Patients
- Comparison of Usage Patterns and Outcomes by Dual Type Calcium Channel Blockers in Patients with Chronic Kidney Disease
- Antihypertensive Effects and Safety of Manidipine in Patients with Essential Hypertension
- Efficacy and Safety of Amlodipine in the Treatment of Essential Hypertension
- Clinical Study on Antihypertensive Effect of Verapamil
