Effect of an L- and T-Type Calcium Channel Blocker on 24-Hour Systolic Blood Pressure and Heart Rate in Hypertensive Patients
- Affiliations
-
- 1Division of Cardiology, Showa University Fujigaoka Hospital, Yokohama, Japan. maco21011969@gmail.com
- 2Department of Ischemic Circulatory Physiology, University of Tokyo, Tokyo, Japan.
- 3Division of Cardiology, Showa University Fujigaoka Hospital, Yokohama, Japan.
- 4Division of Cardiology, Showa University Fujigaoka Rehabilitation Hospital, Yokohama, Japan.
- KMID: 2225015
- DOI: http://doi.org/10.4070/kcj.2012.42.4.231
Abstract
- BACKGROUND AND OBJECTIVES
The aim of this study was to evaluate the effects of an L- and T-type calcium channel blocker (CCB) on 24-hour systolic blood pressure (24-hour SBP) and heart rate (24-hour HR) profiles in essential hypertensive patients.
SUBJECTS AND METHODS
Thirty-seven consecutive patients were enrolled in this study. The 24-hour SBP and HR were recorded before and after treatment with efonidipine (L- and T-type CCB, 40 mg), after waking. Changes in 24-hour SBP and HR and the diurnal to nocturnal SBP ratio were measured. The best-fit curves of changes in SBP and HR were depicted using a periodic function.
RESULTS
The mean 24-hour SBP and HR decreased significantly after treatment. The diurnal to nocturnal SBP ratio in dipper-type hypertension cases decreased from 16.7+/-6.1% to 8.3+/-9.8% (p<0.05), whereas in non-dipper hypertension cases, it increased from 2.3+/-2.9% to 7.7+/-5.1% (p<0.01). The antihypertensive effect was minimal at 5.0 hours after drug administration and it slowly recovered at a constant rate (2.1 mm Hg/h) over 12 hours in dipper cases. The median 24-hour changes in HR in the dipper and non-dipper cases were -2.3/min and -5.4/min, respectively. A continuous reduction in the change in HR was seen from 3.5 to 23 hours after drug administration.
CONCLUSION
The antihypertensive action of efonidipine was characterized by a slow recovery of the SBP decrease at a constant rate (2.1 mm Hg/h) and a non-administration time dependent reduction in 24-hour HR.
MeSH Terms
Figure
-
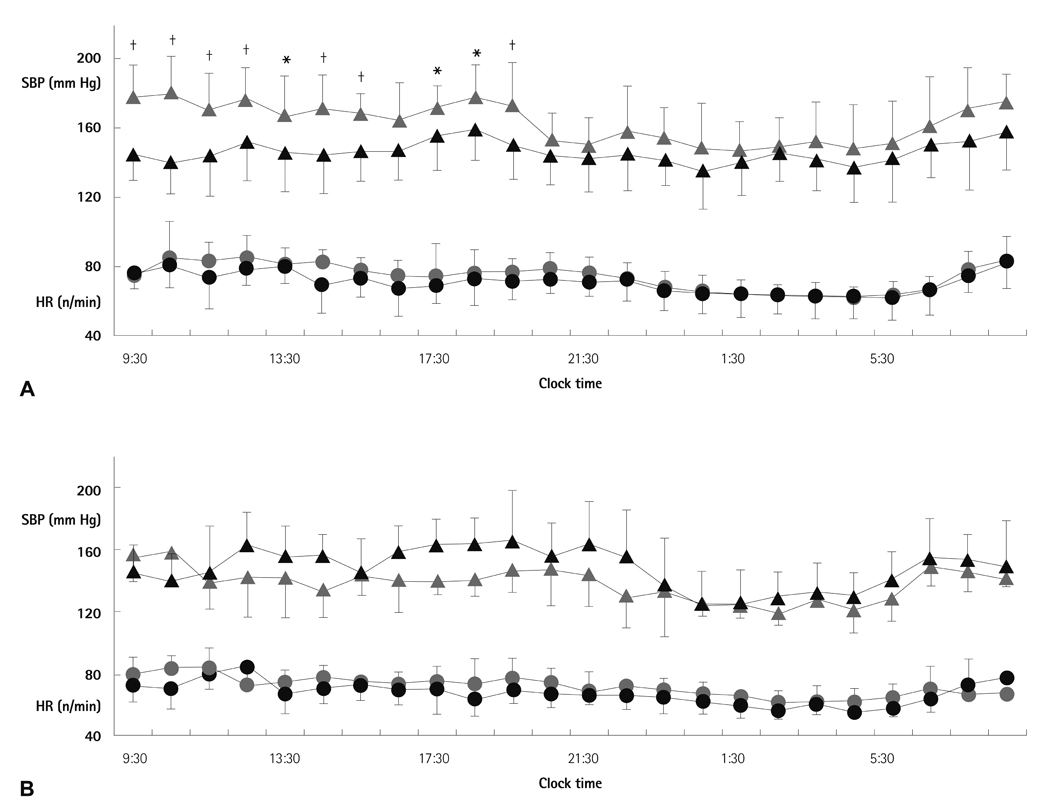
Fig. 1 Alterations in systolic blood pressure (SBP) and heart rate (HR) over 24-hour periods before and after efonidipine administration. A: each 30-minute average value of SBP and HR over a 24-hour time period, measured in patients whose average 24-hour SBP fell by 5 mm Hg or more after administration of the drug (n=29). B: each 30-minute average value of SBP and HR over a 24-hour period measured, in patients whose average 24-hour SBP did not fall after administration of the drug (n=8). The gray shaded horizontal bars in each graph represent the average nocturnal period (10:30 p.m. to 6:30 a.m.) in this study. : average systolic blood pressure before drug administration, : average systolic blood pressure after drug administration, : average heart rate before drug administration, : average heart rate after drug administration. Each value represents an average value±SD. *p<0.05, †p<0.01.

Fig. 2 Changes in diurnal systolic blood pressure (SBP), nocturnal SBP, and diurnal/nocturnal SBP ratio (D/N SBP ratios) in dipper and non-dipper type of hypertensives. In the upper graphs in both groups, the white columns indicate the mean diurnal SBP, and the gray columns indicate the mean nocturnal SBP before and after treatment with efonidipine in dipper cases (n=32) and non-dipper cases (n=5). The D/N SBP ratios are illustrated in the lower panels in both groups. The values expressed in this figure are the mean±SD. After: after treatment, Before: before treatment, (D-N)/D: (mean diurnal SBP-mean nocturnal SBP)/mean diurnal SBP.

Fig. 3 Changes in 24-hour ΔSBP and ΔHR after treatment with efonidipine in dipper and non-dipper cases. The best-fit curves of ΔSBP (upper graph) and ΔHR (lower graph) are shown, where black lines indicate the best-fit curves in dipper cases, and gray lines indicate non-dipper cases. The dotted longitudinal lines indicate the maximum or minimum value in the best-fit curves. Night-time is illustrated by closed transverse bars. The actual values of periodic parameters are illustrated on the right side of the figure. ΔSBP: difference in systolic blood pressure before and after medication every 30 minutes during a day, ΔHR: difference in heart rate before and after medication every 30 minutes during a day, Max: maximum value of the best-fit curve, Min: minimum value of the best-fit curve.
Reference
-
1. Mancia G, de Backer G, Dominiczak A, et al. 2007 guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007. 25:1105–1187.2. Hayashi K, Wakino S, Sugano N, Ozawa Y, Homma K, Saruta T. Ca2+ channel subtypes and pharmacology in the kidney. Circ Res. 2007. 100:342–353.3. Masumiya H, Shijuku T, Tanaka H, Shigenobu K. Inhibition of myocardial L- and T-type Ca2+ currents by efonidipine: possible mechanism for its chronotropic effect. Eur J Pharmacol. 1998. 349:351–357.4. Ge W, Ren J. Combined L-/T-type calcium channel blockers: ready for prime time. Hypertension. 2009. 53:592–594.5. Perez-Reyes E. Molecular physiology of low-voltage-activated t-type calcium channels. Physiol Rev. 2003. 83:117–161.6. Shin HS. T-type Ca2+ channels and absence epilepsy. Cell Calcium. 2006. 40:191–196.7. Ono K, Iijima T. Pathophysiological significance of T-type Ca2+ channels: properties and functional roles of T-type Ca2+ channels in cardiac pacemaking. J Pharmacol Sci. 2005. 99:197–204.8. Ishimitsu T, Kameda T, Akashiba A, et al. Efonidipine reduces proteinuria and plasma aldosterone in patients with chronic glomerulonephritis. Hypertens Res. 2007. 30:621–626.9. Kinoshita H, Kuwahara K, Takano M, et al. T-type Ca2+ channel blockade prevents sudden death in mice with heart failure. Circulation. 2009. 120:743–752.10. Hermida RC, Ayala DE, Portaluppi F. Circadian variation of blood pressure: the basis for the chronotherapy of hypertension. Adv Drug Deliv Rev. 2007. 59:904–922.11. Masuda Y, Takeguchi M, Arakawa C, et al. Antihypertensive and diuretic effects of NZ-105, a novel dihydropyridine derivative. Arch Int Pharmacodyn Ther. 1990. 304:247–264.12. Tanaka H, Shigenobu K. Efonidipine hydrochloride: a dual blocker of L- and T-type Ca2+ channels. Cardiovasc Drug Rev. 2002. 20:81–92.13. Tochikubo O, Ikeda A, Miyajima E, Ishii M. Effects of insufficient sleep on blood pressure monitored by a new multibiomedical recorder. Hypertension. 1996. 27:1318–1324.14. Minami J, Ishimitsu T, Kawano Y, Numabe A, Matsuoka H. Comparison of 24-hour blood pressure, heart rate, and autonomic nerve activity in hypertensive patients treated with cilnidipine or nifedipine retard. J Cardiovasc Pharmacol. 1998. 32:331–336.15. Hermida RC, Ayala DE, Chayan L, Mojon A, Fernandez JR. Administration-time-dependent effects of olmesartan on the ambulatory blood pressure of essential hypertension patients. Chronobiol Int. 2009. 26:61–79.16. Kario K, Pickering TG, Umeda Y, et al. Morning surge in blood pressure as a predictor of silent and clinical cerebrovascular disease in elderly hypertensives: a prospective study. Circulation. 2003. 107:1401–1406.17. Ohtomo N, Kamo T, Watanabe M, Yoneyama K, Tanaka Y, Hayashi R. Power spectral densities of temporal variations of blood pressures. Jpn J Appi Phys. 1996. 35:5571–5582.18. Nakabeppu H, Asada M, Oda T, Shinozaki Y, Yajima T. Plasma and urinary metabolites of efonidipine hydrochloride in man. Xenobiotica. 1996. 26:229–239.19. Yamashita T, Masuda Y, Sakai T, Tanaka S, Kasuya Y. NZ-105, a new 1,4-dihydropyridine derivative: correlation between dihydropyridine receptor binding and inhibition of calcium uptake in rabbit aorta. Jpn J Pharmacol. 1991. 57:337–348.20. Nold G, Herholz C, Sturm M, Hopf R, Lemmer B. Ambulatory blood pressure profiles in essential hypertensives after treatment with a new once daily nifedipine formulation. J Hum Hypertens. 1999. 13:173–177.21. White WB, Saunders E, Noveck RJ, Ferdinand K. Comparative efficacy and safety of nisoldipine extended-release (ER) and amlodipine (CESNA-III study) in African American patients with hypertension. Am J Hypertens. 2003. 16:739–745.22. Fox K, Ford I, Steg PG, Tendera M, Robertson M, Ferrari R. BEAUTIFUL investigators. Heart rate as a prognostic risk factor in patients with coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a subgroup analysis of a randomised controlled trial. Lancet. 2008. 372:817–821.23. Oh IY, Seo MK, Lee HY, et al. Beneficial effect of efonidipine, an L- and T-type dual calcium channel blocker, on heart rate and blood pressure in patients with mild-to-moderate essential hypertension. Korean Circ J. 2010. 40:514–519.24. Saito T, Fujii K, Takizawa T, et al. Effects of the new calcium antagonist efonidipine hydrochloride on resting and exercise hemodynamics in patients with stable effort angina. Arzneimittelforschung. 1996. 46:861–867.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Oral Calcium Channel Blockers on the Ocular Blood Flow
- Beneficial Effect of Efonidipine, an L- and T-Type Dual Calcium Channel Blocker, on Heart Rate and Blood Pressure in Patients With Mild-to-Moderate Essential Hypertension
- Chlorthalidone, not hydrochlorothiazide, is the right diuretic for comparison
- Clinical Study on Antihypertensive Effect of Verapamil
- Efficacy and Safety of Amlodipine in the Treatment of Essential Hypertension
