Hyponatremia and Syndrome of Inappropriate Antidiuretic Hormone Secretion in Kawasaki Disease
- Affiliations
-
- 1Department of Pediatrics, Ewha Womans University School of Medicine, Seoul, Korea. sohn@ewha.ac.kr
- KMID: 1826139
- DOI: http://doi.org/10.4070/kcj.2010.40.10.507
Abstract
- BACKGROUND AND OBJECTIVES
The pathogenesis of hyponatremia (serum sodium <135 mEq/L) in Kawasaki disease (KD) remains unclear. We investigated the clinical significance of hyponatremia, and the role of interleukin (IL)-6 and IL-1beta in the development of hyponatremia and syndrome of inappropriate antidiuretic hormone secretion (SIADH) in KD.
SUBJECTS AND METHODS
Fifty KD patients were prospectively enrolled and analyzed for clinical and laboratory variables according to the presence of hyponatremia or SIADH.
RESULTS
Thirteen KD patients (26%) had hyponatremia and 6 of these had SIADH. In patients with hyponatremia, the percentage of neutrophils (% neutrophils), C-reactive protein (CRP), and N-terminal pro-brain natriuretic peptide (NT-proBNP) were higher than in those without hyponatremia, while serum triiodothyronine (T3) and albumin were lower. Patients with hyponatremia had a higher incidence of intravenous immunoglobulin-resistance but this was not statistically significant. No differences existed between patients with and without SIADH with regard to clinical or laboratory variables and the incidence of IVIG-resistance. Serum sodium inversely correlated with % neutrophils, CRP, and NT-proBNP, and positively correlated with T3 and albumin. Serum IL-6 and IL-1beta levels increased in KD patients and were higher in patients with hyponatremia. Plasma antidiuretic hormone increased in patients with SIADH, which tended to positively correlate with IL-6 and IL-1beta levels.
CONCLUSION
Hyponatremia occurs in KD patients with severe inflammation, while increased IL-6 and IL-1beta may activate ADH secretion, leading to SIADH and hyponatremia in KD.
MeSH Terms
-
C-Reactive Protein
Humans
Hyponatremia
Inappropriate ADH Syndrome
Incidence
Inflammation
Interleukin-6
Interleukins
Mucocutaneous Lymph Node Syndrome
Natriuretic Peptide, Brain
Neutrophils
Peptide Fragments
Plasma
Prospective Studies
Sodium
Triiodothyronine
C-Reactive Protein
Interleukin-6
Interleukins
Natriuretic Peptide, Brain
Peptide Fragments
Sodium
Triiodothyronine
Figure
-
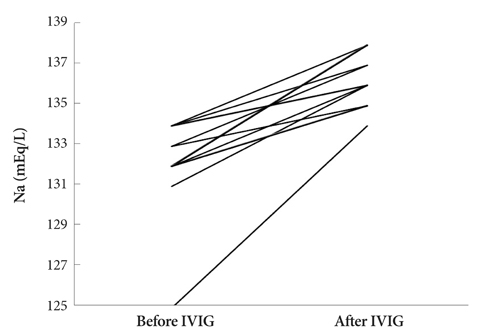
Fig. 1 Changes in serum sodium (Na) level in 13 Kawasaki disease patients with hyponatremia (serum Na <135 mEq/L) before and after intravenous immunoglobulin (IVIG) infusion.

Fig. 2 Correlations between serum sodium (Na) and (A) C-reactive protein (CRP), (B) N-terminal pro-brain natriuretic peptide (NT-proBNP), and (C) triiodothyronine (T3) in 50 patients with acute Kawasaki disease.
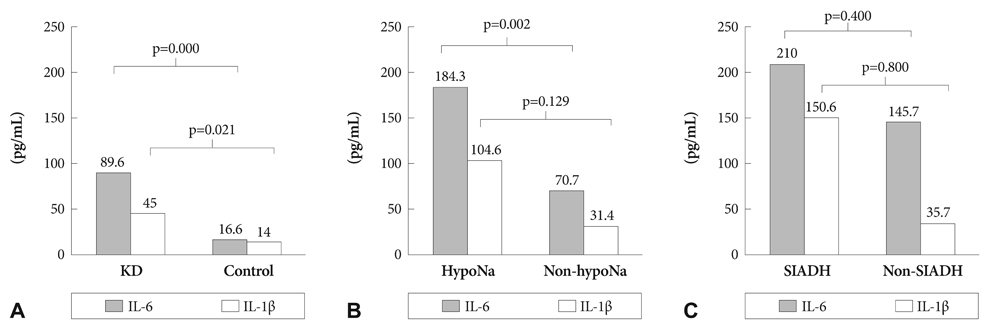
Fig. 3 Comparison in serum levels of interleukin (IL)-6 and IL-1β between (A) Kawasaki disease (KD) patients and the control group (Control), (B) KD patients with (HypoNa) and without (Non-hypoNa) hyponatremia, and (C) hyponatremic KD patients with (SIADH) and without (Non-SIADH). SIADH: syndrome of inappropriate antidiuretic hormone secretion.
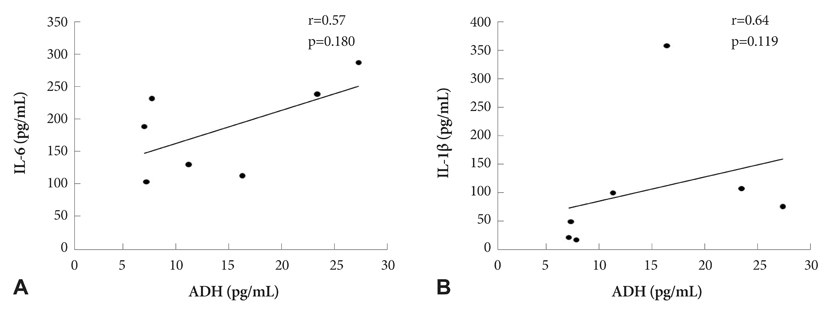
Fig. 4 Correlation of antidiuretic hormone (ADH) with serum levels of (A) interleukin (IL)-6 and (B) IL-1β in 7 Kawasaki disease patients with hyponatremia.
Cited by 1 articles
-
Kawasaki Disease with Acute Respiratory Distress Syndrome after Intravenous Immunoglobulin Infusion
Yu Hyeon Choi, Bong Jin Lee, June Dong Park, Seung Hyo Kim
Korean J Crit Care Med. 2014;29(4):336-340. doi: 10.4266/kjccm.2014.29.4.336.
Reference
-
1. Laxer RM, Petty RE. Hyponatremia in Kawasaki disease. Pediatrics. 1982. 70:655.2. Lapointe N, Chad Z, Lacroix J, et al. Kawasaki disease: association with uveitis in seven patients. Pediatrics. 1982. 69:376–378.3. Mine K, Takaya J, Hasui M, Ikemoto Y, Teraguchi M, Kobayashi Y. A case of Kawasaki disease associated with syndrome of inappropriate secretion of antidiuretic hormone. Acta Paediatr. 2004. 93:1547–1549.4. Nakabayashi Y, Shimizu T. Hyponatremia in Kawasaki disease. Nippon Shoni Jinzobyo Gakkai Zasshi. 2002. 15:83–87.5. Gupta M, Noel GJ, Schaefer M, Friedman D, Bussel J, Johann-Liang R. Cytokine modulation with immune gamma-globulin in peripheral blood of normal children and its implications in Kawasaki disease treatment. J Clin Immunol. 2001. 21:193–199.6. Kim DS. Serum interleukin-6 in Kawasaki disease. Yonsei Med J. 1992. 33:183–188.7. Maury CP, Salo E, Pelkonen P. Circulating interleukin-1beta in patients with Kawasaki disease. N Engl J Med. 1988. 319:1670–1671.8. Suzuki H, Uemura S, Tone S, et al. Effects of immunoglobulin and gamma-interferon on the production of tumour necrosis factor-alpha and interleukin-1beta by peripheral blood monocytes in the acute phase of Kawasaki disease. Eur J Pediatr. 1996. 155:291–296.9. Mastorakos G, Weber JS, Magiakou MA, Gunn H, Chrousos GP. Hypothalamic-pituitary-adrenal axis activation and stimulation of systemic vasopressin secretion by recombinant Interleukin-6 in humans: potential implications for the syndrome of inappropriate vasopressin secretion. J Clin Endocrinol Metab. 1994. 79:934–939.10. Ohta M, Ito S. Hyponatremia and inflammation. Rinsho Byori. 1999. 47:408–416.11. Dajani AS, Taubert KA, Gerber MA, et al. Diagnosis and therapy of Kawasaki disease in children. Circulation. 1993. 87:1776–1780.12. Berry PL, Belsha CW. Hyponatremia. Pediatr Clin North Am. 1990. 37:351–363.13. Watanabe T, Abe Y, Sato S, Uehara Y, Ikeno K, Abe T. Hyponatremia in Kawasaki disease. Pediatr Nephrol. 2006. 21:778–781.14. Research committee on Kawasaki disease. Report of subcommittee on standardization of diagnostic criteria and reporting of coronary artery lesions in Kawasaki disease. 1984. Tokyo: Ministry of Health and Welfare.15. Holliday MA, Segar WE. The maintenance need for water in parenteral fluid therapy. Pediatrics. 1957. 19:823–832.16. Cho HK, Sohn JA, Kim HS, Sohn S. Low T3 syndrome in Kawasaki disease: relation to serum levels of tumor necrosis factor-alpha, interleukin-6 and NT-proBNP. Korean J Pediatr. 2009. 52:234–241.17. Dahdah N, Siles A, Fournier A, et al. Natriuretic peptide as an adjunctive diagnostic test in the acute phase of Kawasaki disease. Pediatr Cardiol. 2009. 30:810–817.18. Lee H, Kim H, Kim HS, Sohn S. NT-proBNP: a new diagnostic screening tool for Kawasaki disease. Korean J Pediatr. 2006. 49:539–544.19. Harada K. Intravenous gamma-globulin treatment in Kawasaki disease. Acta Paediatr Jpn. 1991. 33:805–810.20. Kobayashi T, Inoue Y, Takeuchi K, et al. Prediction of intravenous immunoglobulin unresponsiveness in patients with Kawasaki disease. Circulation. 2006. 113:2606–2612.21. Eisenhut M. Changes in renal sodium transport during a systemic inflammatory response. Pediatr Nephrol. 2006. 21:1487–1488.22. Smith PK, Goldwarer PN. Kawasaki disease in Adelaide: a review. J Paediatr Child Health. 1993. 29:126–131.23. Terai M, Honda T, Yasukawa K, Higashi K, Hamada H, Kohno Y. Prognostic impact of vascular leakage in acute Kawasaki disease. Circulation. 2003. 108:325–330.24. Koyanagi H, Nakamura Y, Yanagawa H. Lower level of serum potassium and higher level of C-reactive protein as an independent risk factor for giant aneurysms in Kawasaki disease. Acta Paediatr. 1998. 87:32–36.25. Boomsma F, van den Meiracker AH. Plasma A- and B-type natriuretic peptides: physiology, methodology and clinical use. Cardiovasc Res. 2001. 51:442–449.26. Fujiwara T, Fujiwara H, Takemura G, et al. Expression and distribution of atrial natriuretic polypeptide in the ventricles of children with myo-carditis and/or myocardial infarction secondary to Kawasaki disease: immunohistochemical study. Am Heart J. 1990. 120:612–618.27. Ohta K, Seno A, Shintani N, et al. Increased levels of urinary interleukin-6 in Kawasaki disease. Eur J Pediatr. 1993. 152:647–649.28. Duke T, Molyneux EM. Intravenous fluids for seriously ill children: time to reconsider. Lancet. 2003. 362:1320–1323.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report of Syndrome of Inappropriate Antidiuretic Hormone Induced by Pregabalin
- A case of syndrome of inappropriate secretion of antidiuretic hormone associated with paroxetine
- Syndrome of Inappropriate Secretion of Antidiuretic Hormone after Lung Transplantation
- Small cell neuroendocrine carcinoma of the uterine cervix presenting with syndrome of inappropriate antidiuretic hormone secretion
- The Effect of Demeclocycline on the Management of Syndrome of Inappropriate Secretion of Antidiuretic Hormone in Brain Injured Patient
