Immunoglobulin G4 Non-Related Sclerosing Disease with Intracardiac Mass Mimicking Mitral Stenosis: Case Report
- Affiliations
-
- 1Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 2Division of Cardiology, Cardiovascular Imaging Center, Cardiac and Vascular Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. dkkim@skku.edu
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Vascular Surgery, Department of Surgery, Cardiovascular Imaging Center, Cardiac and Vascular Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1779428
- DOI: http://doi.org/10.3346/jkms.2013.28.12.1830
Abstract
- The cardiovascular system may be one of the target organs of both immunoglobulin G4 related and non-related systemic multifocal fibrosclerosis. We present a case of IgG4 non-related systemic multifocal fibrosclerosis mimicking mitral stenosis on echocardiography. For a more detailed differential diagnosis, we used multimodal imaging techniques. After surgical biopsy around the abdominal aortic area in the retroperitoneum, histological examination revealed IgG4 non-related systemic multifocal fibrosclerosis. We describe the multimodal imaging used to diagnose IgG4 non-related systemic multifocal fibrosclerosis and a positive response to steroid treatment. There have been no previous case reports of IgG4 non-related systemic multifocal fibrosclerosis with intracardiac involvement. Here, we report a case of IgG4 non-related systemic multifocal fibrosclerosis mimicking mitral stenosis.
Keyword
MeSH Terms
-
Aged
Aorta, Abdominal/pathology
Diagnosis, Differential
Echocardiography
Female
Humans
Immunoglobulin G/*blood/immunology
Magnetic Resonance Imaging
Mitral Valve Stenosis/diagnosis
Myocardium/*pathology
Peritoneum/surgery
Positron-Emission Tomography
Retroperitoneal Fibrosis/*congenital/diagnosis/drug therapy/ultrasonography
Steroids/therapeutic use
Tomography, X-Ray Computed
Immunoglobulin G
Steroids
Figure
-
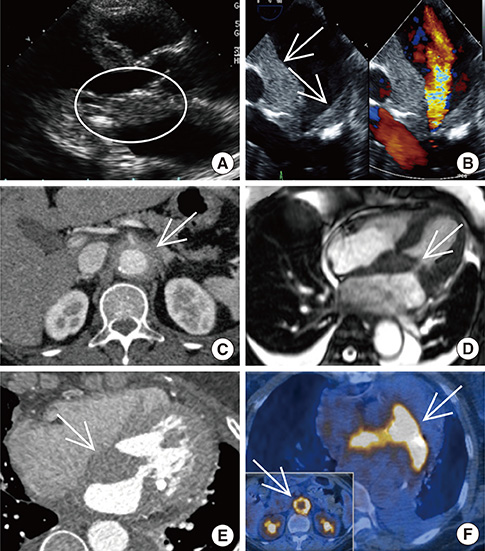
Fig. 1 The main remarks of several imaging modalities before steroid treatment. (A) Parasternal long axis view of TTE demonstrated limited motion of mitral leaflet by attached mass like lesion (white circle). (B) The mid-esophageal 4-chamber view of TEE demonstrated LA mass-like lesion (two white arrows). Color Doppler imaging showed flow acceleration as MS. (C) Transverse view of abdominal CT demonstrated increased wall thickness of the abdominal aorta (white arrow). (D) Cardiac MRI demonstrated wall thickening (white arrow) involving LA and IAS with extension to MV leaflet. (E) Coronary CT angiography showed diffuse soft-tissue infiltration involving LA, IAS, and MV. (F) PET showed LA mass (white arrow) and periabdominal aortic area thickness (white arrow in little figure) increased FDG uptake.

Fig. 2 The histopathologic results by the biopsy of periabdominal aortic mass. (A) Hematoxylin and eosin stained section of the biopsied periabdominal aortic mass demonstrated dense lymphoplasmacytic infiltration and fibrosis. (B) Masson's trichrome stain showed adventitial fibrosis. (Original magnification A, B, ×100). (C) Immunohistochemical staining for IgG. (D) Immunohistochemical staining for CD38. Immunohistochemical staining for IgG4. Below 5% of the plasma cells exhibit this stain. (Original magnification C, ×100; D, ×200). IgG, immunoglobulin G.
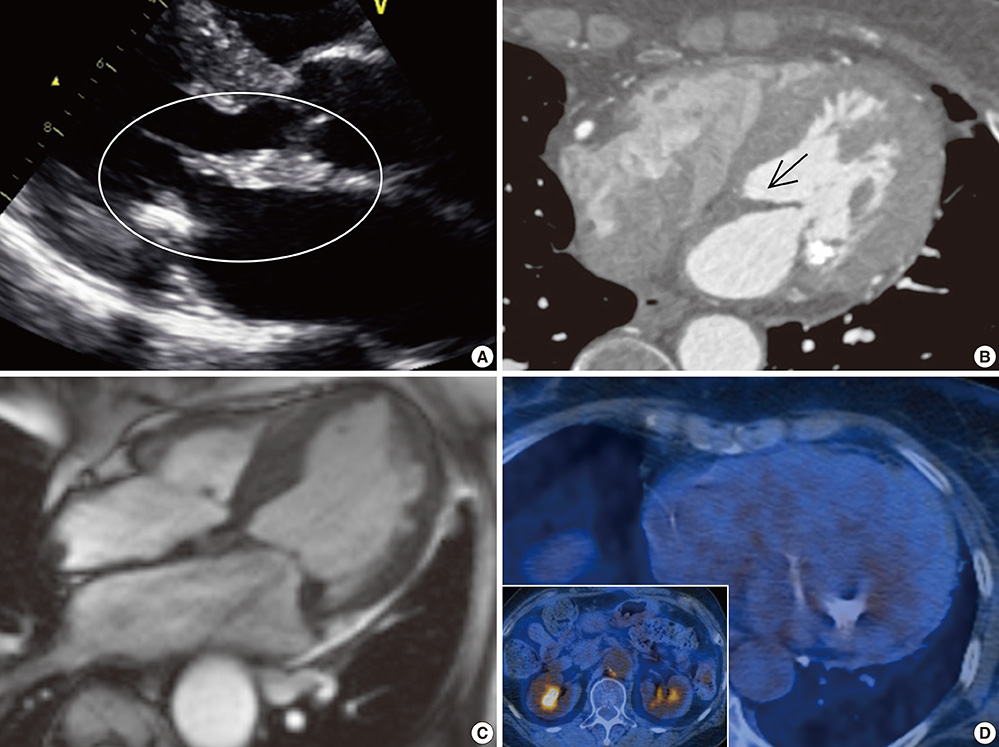
Fig. 3 The improved findings of a few images after steroid treatment for four weeks. (A) Follow-up at the four weeks of steroid treatment showed that the thickness of LA mass decreased (white circle) in TTE. (B) Coronary CT angiography showed interval decreased extent of soft tissue lesion (black arrow) arounding LA after steroid treatment. (C) Cardiac MRI showed the decreased lesion of MV after four weeks from the point of starting steroid treatment. (D) PET did not show any lesion in LA and periabdominal aortic area after six months from the point of starting steroid treatment.
Reference
-
1. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012; 366:539–551.2. Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, Matsui S, Sumida T, Mimori T, Tanaka Y, et al. A novel clinical entity, IgG4-related disease (IgG4RD): general concept and details. Mod Rheumatol. 2012; 22:1–14.3. Masaki Y, Kurose N, Umehara H. IgG4-related disease: a novel lymphoproliferative disorder discovered and established in Japan in the 21st century. J Clin Exp Hematop. 2011; 51:13–20.4. Kamisawa T, Okamoto A. IgG4-related sclerosing disease. World J Gastroenterol. 2008; 14:3948–3955.5. Stone JH, Khosroshahi A, Deshpande V, Chan JK, Heathcote JG, Aalberse R, Azumi A, Bloch DB, Brugge WR, Carruthers MN, et al. Recommendations for the nomenclature of IgG4-related disease and its individual organ system manifestations. Arthritis Rheum. 2012; 64:3061–3067.6. Zen Y, Nakanuma Y. IgG4-related disease: a cross-sectional study of 114 cases. Am J Surg Pathol. 2010; 34:1812–1819.7. Masaki Y, Dong L, Kurose N, Kitagawa K, Morikawa Y, Yamamoto M, Takahashi H, Shinomura Y, Imai K, Saeki T, et al. Proposal for a new clinical entity, IgG4-positive multiorgan lymphoproliferative syndrome: analysis of 64 cases of IgG4-related disorders. Ann Rheum Dis. 2009; 68:1310–1315.8. Umehara H. A new clinical entity: IgG4-related disease (IgG4-RD) discovered in the 21st century. Intern Med. 2012; 51:821–822.9. Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, Matsui S, Yoshino T, Nakamura S, Kawa S, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012; 22:21–30.10. Okazaki K, Umehara H. Are classification criteria for IgG4-RD now possible? the concept of IgG4-related disease and proposal of comprehensive diagnostic criteria in Japan. Int J Rheumatol. 2012; 2012:357071.11. Kasashima S, Zen Y, Kawashima A, Endo M, Matsumoto Y, Kasashima F. A new clinicopathological entity of IgG4-related inflammatory abdominal aortic aneurysm. J Vasc Surg. 2009; 49:1264–1271.12. Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike M, Tsuruta K, Okamoto A, Egawa N, Nakajima H. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol. 2003; 38:982–984.13. Stone JR. Aortitis, periaortitis, and retroperitoneal fibrosis, as manifestations of IgG4-related systemic disease. Curr Opin Rheumatol. 2011; 23:88–94.14. Ishizaka N, Sakamoto A, Imai Y, Terasaki F, Nagai R. Multifocal fibrosclerosis and IgG4-related disease involving the cardiovascular system. J Cardiol. 2012; 59:132–138.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Immunoglobulin G4-Related Sclerosing Disease Mimicking Lung Cancer
- Immunoglobulin G4-related sclerosing cholangitis
- Two Cases of Immunoglobulin G4-Related Sclerosing Disease Mimicking Nasopharyngeal Carcinoma
- A Case of Immunoglobulin G4-Related Sclerosing Disease of the Paranasal Sinus Mimicking Nasal Malignancy
- Immunoglobulin G4-Related Systemic Sclerosing Disease: A Case Involving the Ureter and Kidney
