Sodium Chloride Aggravates Arthritis via Th17 Polarization
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 2Division of Rheumatology, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. juji@catholic.ac.kr
- KMID: 2428282
- DOI: http://doi.org/10.3349/ymj.2019.60.1.88
Abstract
- PURPOSE
Sodium chloride (NaCl) has been proposed as a driving factor in autoimmune diseases through the induction of pathogenic CD4+ T helper cells that produce interleukin-17 (Th17 cells). This study investigated the effects of NaCl on inflammatory arthritis in mice and humans.
MATERIALS AND METHODS
Collagen-induced arthritis (CIA) mice were fed a normal or high-salt diet ad libitum, and clinical and histologic features of arthritis were evaluated. The proportion of Th17 cells in the spleens of CIA mice fed a normal or high-salt diet was evaluated by flow cytometry, and the expression of IL-17 in joints and intestines was determined by immunohistochemical staining. We also analyzed the effect of NaCl on Th17 differentiation from peripheral blood monocytes of patients with rheumatoid arthritis (RA) and osteoarthritis (OA) and evaluated the contents of sodium and IL-17 in the synovial fluid of RA and OA patients.
RESULTS
NaCl increased murine and human Th17 cell differentiation in a dose-dependent manner. Clinical and histological arthritis was more severe in the high-salt-fed CIA mice, compared to control CIA mice. The proportion of Th17 cells among splenocytes was higher in CIA mice fed a high-salt diet. Expression of synovial and intestinal IL-17 was also higher in high-salt-fed CIA mice. Comparison of synovial fluid between RA patients and OA patients revealed that Na+ and IL-17 were more abundant in RA synovial fluid.
CONCLUSION
This study suggests that NaCl can aggravate arthritis by affecting Th17 differentiation. Accordingly, limiting salt intake may be helpful for treating inflammatory arthritis, such as RA.
MeSH Terms
Figure
-
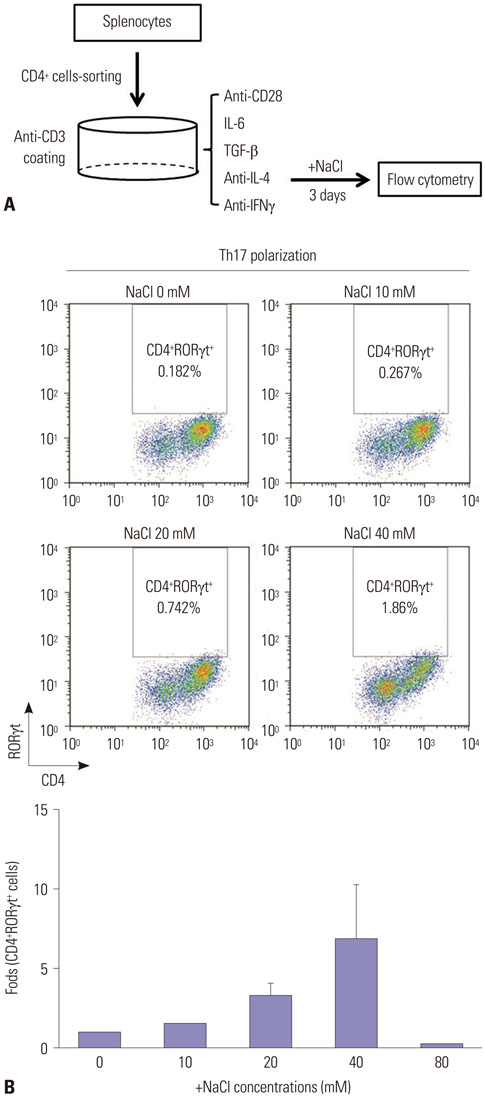
Fig. 1 NaCl induces Th17 differentiation in vitro. (A) A schematic diagram for evaluating the effect of salt on Th17 differentiation. Naïve CD4+ T cells isolated from the spleens of DBA/1J mice were cultured under Th17-polarizing conditions in the absence or presence of NaCl at different concentrations (10, 20, 40, and 80 mM) for 3 days. (B) Representative flow cytometry plots of differentiated Th17 cells at different NaCl concentrations. The displayed numbers are the percentage of CD4+RORγt+-labeled cells. Fold increases were calculated as the percentage of CD4+RORγt+ Th17 cells relative to the percentage in the NaCl-deficient condition. Data are representative of three independent experiments and are expressed as mean±SEM.
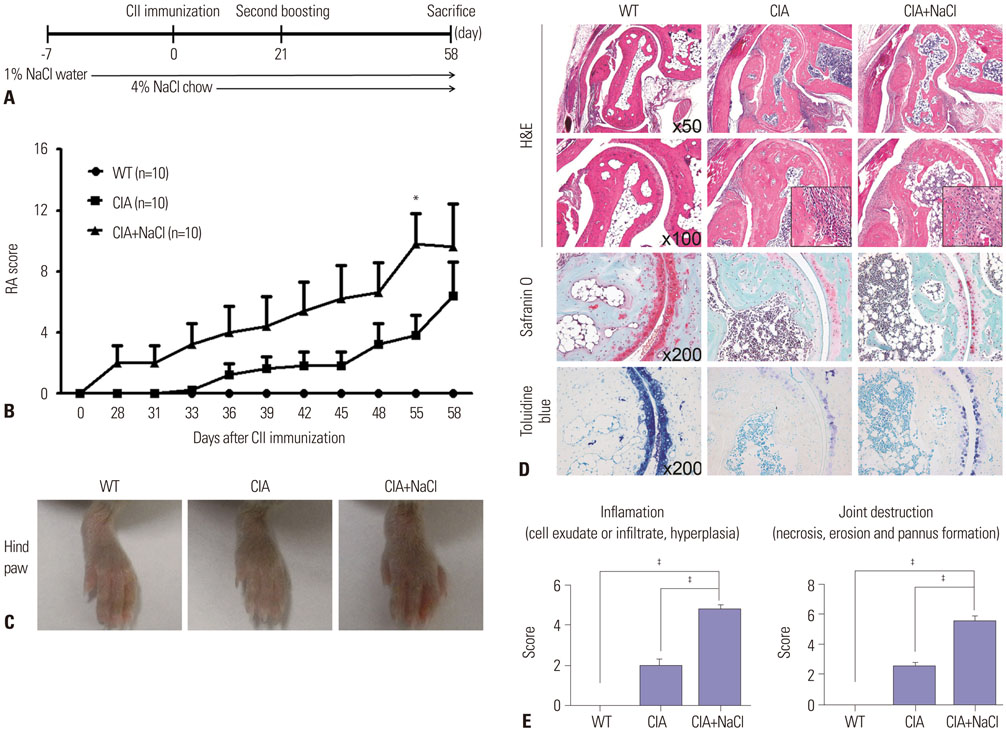
Fig. 2 High-salt diet aggravates inflammatory arthritis in CIA mice. (A) Time schedule for salt ingestion in CIA mice. Salt-containing water and chow were started 1 week before and at the time of CII immunization, respectively. (B) Mean arthritis scores in wild-type mice (WT), CIA mice (CIA), and CIA mice fed a high-salt diet (CIA+NaCl). Arthritis of each paw was scored from 0 (no swelling) to 4 (erythema and severe swelling encompassing the ankle and foot). The arthritis score is the sum of the scores for the four paws. Data represent the mean arthritis score±SEM. *p<0.05. (C) Representative photographs of hind paws in control mice and CIA mice fed a high-salt diet. The hind paws of WT, CIA, and CIA+NaCl showed a different degree of swelling at day 58 after primary CII immunization. (D) Histological analysis of tarsal joints in control mice and CIA mice fed a high-salt diet. The tissue sections obtained at 58 days were stained with hematoxylin and eosin (H&E), Safranin O, and toluidine blue. The magnifications are indicated in the right bottom corner. (E) The mean histological score of the tarsal joints in each group. Inflammation and joint destruction were scored on a scale of 0–3 by three independent examiners. The data represent the mean histological score±SEM. ‡p<0.001.

Fig. 3 NaCl-rich condition primes Th17 polarization in mice with CIA. (A) Flow cytometry analysis of naïve CD4+ T cells in spleens isolated from control CIA mice (CIA) and high-salt-fed CIA mice (CIA+NaCl). Representative plots of Th17 population among naïve CD4+ T cells in both groups are presented, and fold increases were calculated as the percentage of CD4+RORγt+ Th17 cells relative to the percentage in control CIA mice. (B) Flow cytometry analysis of naïve CD4+ T cells isolated from CIA and CIA+NaCl mice cultured under Th17-polarizing conditions. Splenocytes were isolated from CIA mice fed a normal or a high-salt diet to evaluate the priming effect of NaCl on Th17 differentiation. Purified naïve CD4+ T cells were cultured under Th17 differentiating condition for 3 days. Representative plots of differentiated CD4+IL-17A+Th17 cells from naïve CD4+ T cells isolated from both groups were presented, and fold increases were calculated as the percentage of CD4+IL-17A+ Th17 cells relative to the percentage in the control CIA group. Data are representative of three independent experiments and are expressed as mean±SEM. *p<0.05.

Fig. 4 Salt intake increases IL-17 expression in the synovium and gut of CIA mice. (A–C) Expression of IL-17A in the joint synovium, small intestine, and large intestine in WT mice and CIA mice fed a normal diet (CIA) or a high-salt diet (CIA+NaCl). Immunohistochemical staining with anti-IL-17A antibodies was performed in tissue sections of joint (A), small intestine (B), and large intestine (C) obtained from experimental animals on day 58. Representative images in each group are shown, and the area with cellular deposition was enlarged. The magnification is presented in the right bottom corner, and scale bars indicate 100 µm. (D) Quantification of IL-17+ cells in the joint and small intestine and IL-17+ spots in the large intestine observed in a low power field (LPF) (×100 or ×200 as presented in the graphs). The number of IL-17+ cells or spots was determined by three independent examiners. The data are expressed as mean±SEM. *p<0.05.
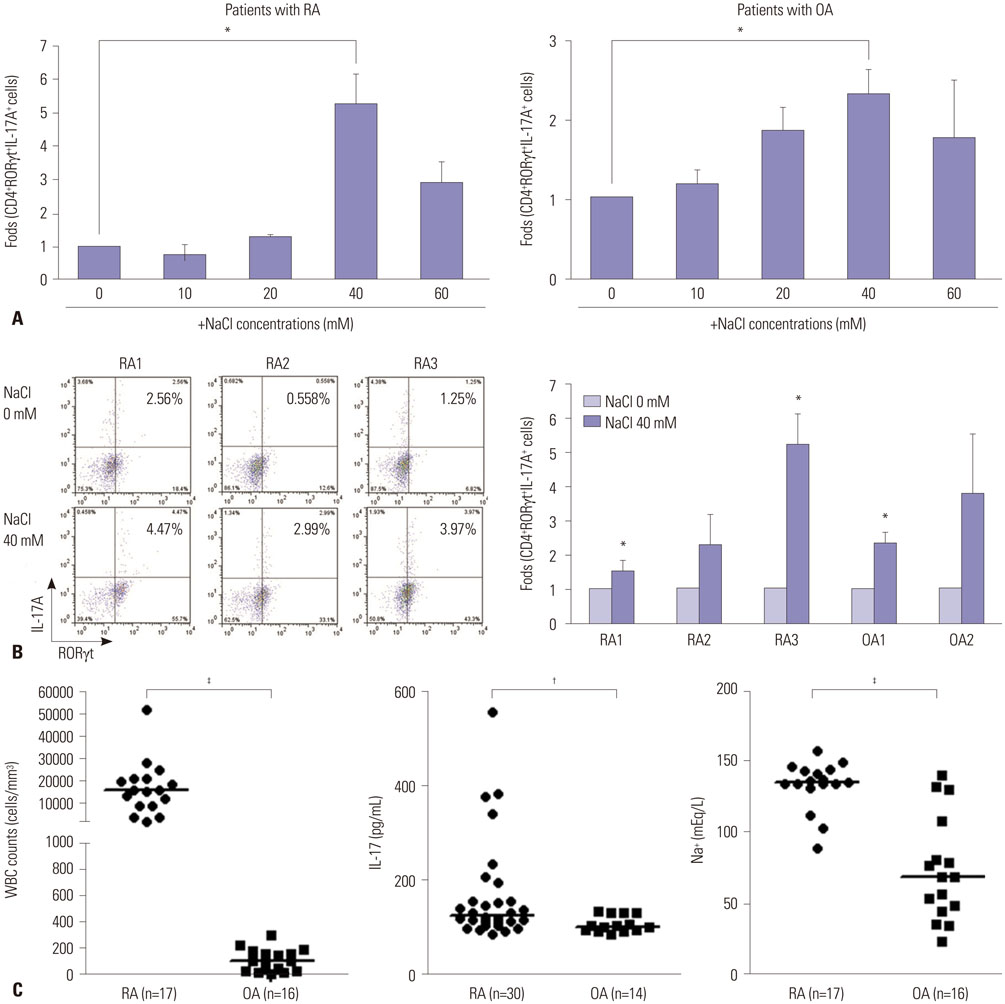
Fig. 5 Synovial fluid from RA patients contained higher levels of sodium and IL-17 compared with those from OA patients. (A) Changes in Th17 differentiation from human CD4+ T cells after treatment with various doses of NaCl. Naïve CD4+ T cells from peripheral blood were cultured under Th17-polarizing conditions with or without NaCl at different concentrations (10, 20, 40, and 60 mM) for 3 days. RORγt+IL-17A+ Th17 cells were detected by flow cytometry. Fold differences at the different concentrations were expressed relative to the NaCl-deficient condition. (B) The effect of NaCl on Th17 differentiation in human cells obtained from RA and OA patients. Representative flow cytometry plots for Th17 differentiation at NaCl 0 mM and 40 mM are shown in patients with RA (n=3) and OA (n=2). Fold increases in differentiated Th17 cells were expressed relative to the NaCl-deficient condition. The graph represents the data from individual patients. Data represent the mean of three independent experiments±SEM. *p<0.05. (C) Characteristics of synovial fluid obtained from RA patients and OA patients. Leukocyte count and sodium concentration in synovial fluid were measured by routine laboratory methods. IL-17 level in the synovial fluid was determined by ELISA. Horizontal bars for analysis of synovial fluid indicate the median of all values in a group. †p<0.01, ‡p<0.001. RA, rheumatoid arthritis; OA, osteoarthritis; WBC, white blood cell.
Reference
-
1. Miossec P, Korn T, Kuchroo VK. Interleukin-17 and type 17 helper T cells. N Engl J Med. 2009; 361:888–898.
Article2. McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med. 2011; 365:2205–2219.
Article3. Proudman SM, James MJ, Spargo LD, Metcalf RG, Sullivan TR, Rischmueller M, et al. Fish oil in recent onset rheumatoid arthritis: a randomised, double-blind controlled trial within algorithm-based drug use. Ann Rheum Dis. 2015; 74:89–95.
Article4. Park Y, Lee A, Shim SC, Lee JH, Choe JY, Ahn H, et al. Effect of n-3 polyunsaturated fatty acid supplementation in patients with rheumatoid arthritis: a 16-week randomized, double-blind, placebo-controlled, parallel-design multicenter study in Korea. J Nutr Biochem. 2013; 24:1367–1372.
Article5. Salesi M, Farajzadegan Z. Efficacy of vitamin D in patients with active rheumatoid arthritis receiving methotrexate therapy. Rheumatol Int. 2012; 32:2129–2133.
Article6. McKellar G, Morrison E, McEntegart A, Hampson R, Tierney A, Mackle G, et al. A pilot study of a Mediterranean-type diet intervention in female patients with rheumatoid arthritis living in areas of social deprivation in Glasgow. Ann Rheum Dis. 2007; 66:1239–1243.
Article7. Lahiri M, Morgan C, Symmons DP, Bruce IN. Modifiable risk factors for RA: prevention, better than cure? Rheumatology (Oxford). 2012; 51:499–512.
Article8. Kleinewietfeld M, Manzel A, Titze J, Kvakan H, Yosef N, Linker RA, et al. Sodium chloride drives autoimmune disease by the induction of pathogenic TH17 cells. Nature. 2013; 496:518–522.
Article9. Wu C, Yosef N, Thalhamer T, Zhu C, Xiao S, Kishi Y, et al. Induction of pathogenic TH17 cells by inducible salt-sensing kinase SGK1. Nature. 2013; 496:513–517.
Article10. Meng F, Yamagiwa Y, Taffetani S, Han J, Patel T. IL-6 activates serum and glucocorticoid kinase via p38alpha mitogen-activated protein kinase pathway. Am J Physiol Cell Physiol. 2005; 289:C971–C981.11. Masuda K, Masuda R, Neidhart M, Simmen BR, Michel BA, Müller-Ladner U, et al. Molecular profile of synovial fibroblasts in rheumatoid arthritis depends on the stage of proliferation. Arthritis Res. 2002; 4:R8.12. Yoon HJ, You S, Yoo SA, Kim NH, Kwon HM, Yoon CH, et al. NFAT5 is a critical regulator of inflammatory arthritis. Arthritis Rheum. 2011; 63:1843–1852.
Article13. Brand DD, Latham KA, Rosloniec EF. Collagen-induced arthritis. Nat Protoc. 2007; 2:1269–1275.
Article14. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988; 31:315–324.
Article15. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2010; 69:1580–1588.
Article16. Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986; 29:1039–1049.
Article17. Hückel M, Schurigt U, Wagner AH, Stöckigt R, Petrow PK, Thoss K, et al. Attenuation of murine antigen-induced arthritis by treatment with a decoy oligodeoxynucleotide inhibiting signal transducer and activator of transcription-1 (STAT-1). Arthritis Res Ther. 2006; 8:R17.18. Machnik A, Neuhofer W, Jantsch J, Dahlmann A, Tammela T, Machura K, et al. Macrophages regulate salt-dependent volume and blood pressure by a vascular endothelial growth factor-C-dependent buffering mechanism. Nat Med. 2009; 15:545–552.
Article19. Müller S, Quast T, Schröder A, Hucke S, Klotz L, Jantsch J, et al. Salt-dependent chemotaxis of macrophages. PLoS One. 2013; 8:e73439.
Article20. Garrido-Mesa N, Algieri F, Rodríguez Nogales A, Gálvez J. Functional plasticity of Th17 cells: implications in gastrointestinal tract function. Int Rev Immunol. 2013; 32:493–510.
Article21. Kamada N, Núñez G. Role of the gut microbiota in the development and function of lymphoid cells. J Immunol. 2013; 190:1389–1395.
Article22. Sommer F, Bäckhed F. The gut microbiota--masters of host development and physiology. Nat Rev Microbiol. 2013; 11:227–238.
Article23. Wu HJ, Ivanov II, Darce J, Hattori K, Shima T, Umesaki Y, et al. Gut-residing segmented filamentous bacteria drive autoimmune arthritis via T helper 17 cells. Immunity. 2010; 32:815–827.
Article24. Lee YK, Menezes JS, Umesaki Y, Mazmanian SK. Proinflammatory T-cell responses to gut microbiota promote experimental autoimmune encephalomyelitis. Proc Natl Acad Sci U S A. 2011; 108:Suppl 1. 4615–4622.
Article25. Go WY, Liu X, Roti MA, Liu F, Ho SN. NFAT5/TonEBP mutant mice define osmotic stress as a critical feature of the lymphoid microenvironment. Proc Natl Acad Sci U S A. 2004; 101:10673–10678.
Article26. Junger WG, Liu FC, Loomis WH, Hoyt DB. Hypertonic saline enhances cellular immune function. Circ Shock. 1994; 42:190–196.27. Junger WG, Hoyt DB, Hamreus M, Liu FC, Herdon-Remelius C, Junger W, et al. Hypertonic saline activates protein tyrosine kinases and mitogen-activated protein kinase p38 in T-cells. J Trauma. 1997; 42:437–443.
Article28. Coimbra R, Junger WG, Liu FC, Loomis WH, Hoyt DB. Hypertonic/ hyperoncotic fluids reverse prostaglandin E2 (PGE2)-induced T-cell suppression. Shock. 1995; 4:45–49.
Article29. Monteleone I, Marafini I, Dinallo V, Di Fusco D, Troncone E, Zorzi F, et al. Sodium chloride-enriched diet enhanced inflammatory cytokine production and exacerbated experimental colitis in mice. J Crohns Colitis. 2017; 11:237–245.
Article30. Hernandez AL, Kitz A, Wu C, Lowther DE, Rodriguez DM, Vudattu N, et al. Sodium chloride inhibits the suppressive function of FOXP3+ regulatory T cells. J Clin Invest. 2015; 125:4212–4222.
Article31. Wu C, Chen Z, Xiao S, Thalhamer T, Madi A, Han T, et al. SGK1 governs the reciprocal development of Th17 and regulatory T cells. Cell Rep. 2018; 22:653–665.
Article32. Platten M, Youssef S, Hur EM, Ho PP, Han MH, Lanz TV, et al. Blocking angiotensin-converting enzyme induces potent regulatory T cells and modulates TH1- and TH17-mediated autoimmunity. Proc Natl Acad Sci U S A. 2009; 106:14948–14953.
Article33. Crestani S, Gasparotto Júnior A, Marques MC, Sullivan JC, Webb RC, da Silva-Santos JE. Enhanced angiotensin-converting enzyme activity and systemic reactivity to angiotensin II in normotensive rats exposed to a high-sodium diet. Vascul Pharmacol. 2014; 60:67–74.
Article34. Chen LW, Huang HL, Lee IT, Hsu CM, Lu PJ. Hypertonic saline enhances host defense to bacterial challenge by augmenting Toll-like receptors. Crit Care Med. 2006; 34:1758–1768.
Article35. Chen LW, Su MT, Chen PH, Liu WC, Hsu CM. Hypertonic saline enhances host defense and reduces apoptosis in burn mice by increasing toll-like receptors. Shock. 2011; 35:59–66.
Article36. Gaddy JA, Radin JN, Loh JT, Zhang F, Washington MK, Peek RM Jr, et al. High dietary salt intake exacerbates Helicobacter pyloriinduced gastric carcinogenesis. Infect Immun. 2013; 81:2258–2267.
Article37. Leung WK, Wu KC, Wong CY, Cheng AS, Ching AK, Chan AW, et al. Transgenic cyclooxygenase-2 expression and high salt enhanced susceptibility to chemical-induced gastric cancer development in mice. Carcinogenesis. 2008; 29:1648–1654.
Article38. Zhu H, Pollock NK, Kotak I, Gutin B, Wang X, Bhagatwala J, et al. Dietary sodium, adiposity, and inflammation in healthy adolescents. Pediatrics. 2014; 133:e635–e642.
Article39. Farez MF, Fiol MP, Gaitán MI, Quintana FJ, Correale J. Sodium intake is associated with increased disease activity in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2015; 86:26–31.
Article40. Zou YF, Xu JH, Tao JH, Xu SQ, Liu S, Chen SY, et al. Impact of environmental factors on efficacy of glucocorticoids in Chinese population with systemic lupus erythematosus. Inflammation. 2013; 36:1424–1430.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of Sodium Chloride on Biology of Catenaria anguillulae
- Role of Intravenous Sodium Bicarbonate and Oral N-acetylcysteine in Radiocontrast-Induced Nephropathy
- Erratum: Response of the Higher Basidiomycetic Ganoderma resinaceum to Sodium Chloride Stress
- Response of the Higher Basidiomycetic Ganoderma resinaceum to Sodium Chloride Stress
- Ciglitazone, a Peroxisome Proliferator-Activated Receptor Gamma Ligand, Inhibits Proliferation and Differentiation of Th17 Cells
