Pulmonary Nodular Lymphoid Hyperplasia with Mass-Formation: Clinicopathologic Characteristics of Nine Cases and Review of the Literature
- Affiliations
-
- 1Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hanjho@skku.edu
- 2Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2417804
- DOI: http://doi.org/10.4132/jptm.2018.04.27
Abstract
- BACKGROUND
Pulmonary nodular lymphoid hyperplasia (PNLH) is a non-neoplastic pulmonary lymphoid disorder that can be mistaken for malignancy on radiography. Herein, we present nine cases of PNLH, emphasizing clinicoradiological findings and histological features.
METHODS
We analyzed radiological and clinicopathological features from the electronic medical records of nine patients (eight females and one male) diagnosed with PNLH. IgG and IgG4 immunohistochemical staining was performed in three patients.
RESULTS
Two of the nine patients had experienced tuberculosis 40 and 30 years prior, respectively. Interestingly, none were current smokers, although two were ex-smokers. Three patients complaining of persistent cough underwent computed tomography of the chest. PNLH was incidentally discovered in five patients during examination for other reasons. The remaining patient was diagnosed with the disease following treatment for pneumonia. Imaging studies revealed consolidation or a mass-like lesion in eight patients. First impressions included invasive adenocarcinoma and mucosal-associated lymphoid tissue"’type lymphoma. Aspergillosis was suspected in the remaining patient based on radiological images. Resection was performed in all patients. Microscopically, the lesions consisted of nodular proliferation of reactive germinal centers accompanied by infiltration of neutrophils and macrophages in various degrees and surrounding fibrosis. Ultimately, all nine patients were diagnosed with PNLH and showed no evidence of recurrence on follow-up.
CONCLUSIONS
PNLH is an uncommon but distinct entity with a benign nature, and understanding the radiological and clinicopathological characteristics of PNLH is important.
MeSH Terms
Figure
-

Fig. 1. Radiological images (chest computed tomography) of three patients before surgery. (A) Image from patient 3 shows the extent of a 58-mm subsolid lesion in the lingular division of the left upper lobe. (B) Image from patient 7 shows a wide ground-glass opacity lesion in the superior segment of the left lower lobe. (C) Image from patient 9 shows an 18-mm irregular nodular lesion with strong enhancement in the posterior basal segment of the right lower lobe.

Fig. 2. Gross findings of pulmonary nodular lymphoid hyperplasia. (A) Gross image from patient 3 shows a relatively well-circumscribed grayish-white mass-forming lesion with firm consistency. (B) Gross image from patient 7 displays a well-defined lesion with soft-to-firm consistency
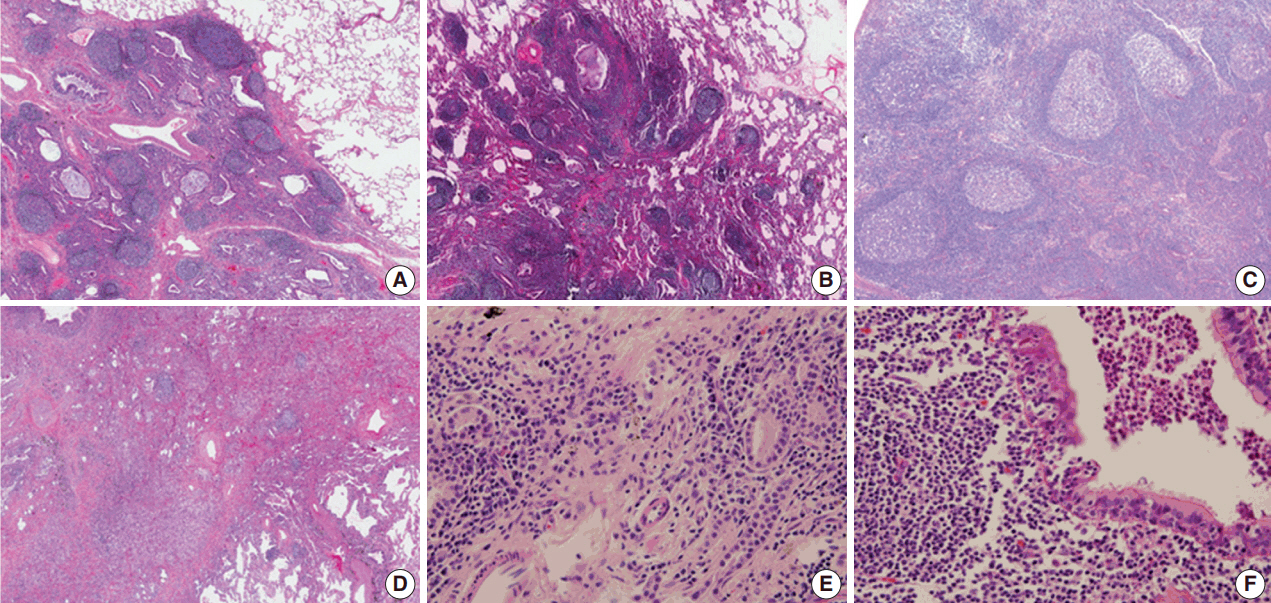
Fig. 3. Histopathological features on hematoxylin and eosin slides of pulmonary nodular lymphoid hyperplasia. (A) In patient 2, a well-circumscribed lesion was observed. The lesion consisted of reactive germinal centers with septal fibrosis, moderate infiltration of neutrophils, and a few macrophages. (B) In patient 4, the lesion was relatively well-defined with irregular borders and rare fibrosis. The lesion was composed of reactive germinal centers with marked infiltration of macrophages. A fungal ball was present in the bronchus at the upper portion of the image and was confirmed using Grocott's methenamine silver stain and Periodic acid–Schiff stain (not shown). (C) In patient 6, the lesion was composed of scattered reactive germinal centers with moderate infiltration of macrophages. No fibrous septum was present. (D) In patient 5, a relatively well-demarcated lesion with irregular border was observed. The lesion consisted of a few reactive germinal centers with fibrosis and marked infiltration of macrophages. (E) In patient 4, the lesion showed moderate infiltration of plasma cells between germinal centers. However, storiform fibrosis or obliterative phlebitis was not detected. (F) Patient 1 showed a mild form of lymphoepithelial lesion. However, the lesion was not extensive or destructive, suggesting extranodal marginal zone lymphoma of mucosal-associated lymphoid tissue.

Fig. 4. Immunohistochemical (IHC) results of pulmonary nodular lymphoid hyperplasia. IHC staining using CD20 (A) and CD3 (B) showed that the lesion in patient 2 had several well-preserved germinal centers with mixed inter-follicular T-cells. (C) Ki-67 IHC staining showed high proliferative activity in the germinal center. IHC staining using CD3 (D) and CD20 (E) showed an inter-follicular T-cell zone and germinal center in the lesion in patient 6, confirming a diffuse pattern. (F, G) Additionally, the inter-follicular and germinal centers were IHC stained with BCL2 and BCL6. (H, I) IHC staining of kappa and lambda light chains indicated a polyclonal population.

Fig. 5. IgG4:IgG ratio of pulmonary nodular lymphoid hyperplasia. The IgG4:IgG ratio varied in this study. The ratio in case 1 was less than 0.1 (A, IgG; B, IgG4). The ratios in case 5 (C, IgG; D, IgG4) and case 6 (E, IgG; F, IgG4) were approximately 0.1–0.2, which is not compatible with IgG4-related disease.
Cited by 1 articles
-
Utilizing Immunoglobulin G4 Immunohistochemistry for Risk Stratification in Patients with Papillary Thyroid Carcinoma Associated with Hashimoto Thyroiditis
Faridul Haq, Gyeongsin Park, Sora Jeon, Mitsuyoshi Hirokawa, Chan Kwon Jung
Endocrinol Metab. 2024;39(3):468-478. doi: 10.3803/EnM.2024.1923.
Reference
-
1. Travis WD, Galvin JR. Non-neoplastic pulmonary lymphoid lesions. Thorax. 2001; 56:964–71.2. Guinee DG Jr. Update on nonneoplastic pulmonary lymphoproliferative disorders and related entities. Arch Pathol Lab Med. 2010; 134:691–701.
Article3. Yi E, Aubry MC. Pulmonary pseudoneoplasms. Arch Pathol Lab Med. 2010; 134:417–26.
Article4. Saltzstein SL. Pulmonary malignant lymphomas and pseudolymphomas: classification, therapy, and prognosis. Cancer. 1963; 16:928–55.
Article5. Kradin RL, Mark EJ. Benign lymphoid disorders of the lung, with a theory regarding their development. Hum Pathol. 1983; 14:857–67.
Article6. Abbondanzo SL, Rush W, Bijwaard KE, Koss MN. Nodular lymphoid hyperplasia of the lung: a clinicopathologic study of 14 cases. Am J Surg Pathol. 2000; 24:587–97.7. Sirajuddin A, Raparia K, Lewis VA, et al. Primary pulmonary lymphoid lesions: radiologic and pathologic findings. Radiographics. 2016; 36:53–70.
Article8. Poletti V, Ravaglia C, Tomassetti S, et al. Lymphoproliferative lung disorders: clinicopathological aspects. Eur Respir Rev. 2013; 22:427–36.
Article9. Arcadu A, Moua T, Yi ES, Ryu JH. Lymphoid interstitial pneumonia and other benign lymphoid disorders. Semin Respir Crit Care Med. 2016; 37:406–20.
Article10. Begueret H, Vergier B, Parrens M, et al. Primary lung small B-cell lymphoma versus lymphoid hyperplasia: evaluation of diagnostic criteria in 26 cases. Am J Surg Pathol. 2002; 26:76–81.11. Tashtoush B, Okafor NC, Ramirez JF, Smolley L. Follicular bronchiolitis: a literature review. J Clin Diagn Res. 2015; 9:OE01–5.
Article12. Guinee DG Jr, Franks TJ, Gerbino AJ, Murakami SS, Acree SC, Koss MN. Pulmonary nodular lymphoid hyperplasia (pulmonary pseudolymphoma): the significance of increased numbers of IgG4-positive plasma cells. Am J Surg Pathol. 2013; 37:699–709.13. Bois MC, Sekiguchi H, Ryu JH, Yi ES. No definite clinical features of immunoglobulin G4-related disease in patients with pulmonary nodular lymphoid hyperplasia. Hum Pathol. 2017; 59:80–6.
Article14. Atzeni F, Gerardi MC, Barilaro G, Masala IF, Benucci M, Sarzi-Puttini P. Interstitial lung disease in systemic autoimmune rheumatic diseases: a comprehensive review. Expert Rev Clin Immunol. 2018; 14:69–82.
Article15. Mittoo S, Gelber AC, Christopher-Stine L, Horton MR, Lechtzin N, Danoff SK. Ascertainment of collagen vascular disease in patients presenting with interstitial lung disease. Respir Med. 2009; 103:1152–8.
Article16. Song MK, Seol YM, Park YE, et al. Pulmonary nodular lymphoid hyperplasia associated with Sjogren's syndrome. Korean J Intern Med. 2007; 22:192–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Small Intestinal Nodular Lymphoid Hyperplasia
- A Case of Primary Jejunal Malignant Lymphoma Associated with Nodular Lymphoid Hyperplasia
- Surgical Treatment of the Pulmonary Nodular Lymphoid Hyperplasia: A case report
- Pulmonary Nodular Lymphoid Hyperplasia in a 33-Year-Old Woman
- Pulmonary Nodular Lymphoid Hyperplasia Associated with Sj?gren's Syndrome
