Diffusion Tensor Imaging in Inflammatory and Neoplastic Intramedullary Spinal Cord Lesions: Focusing on Fiber Tracking
- Affiliations
-
- 1Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea. joonwoo2@gmail.com
- KMID: 2367858
- DOI: http://doi.org/10.3348/jksr.2017.76.2.111
Abstract
- PURPOSE
Inflammatory and neoplastic intramedullary spinal cord lesions have overlapping clinical features, and it is occasionally difficult to distinguish one from the other on conventional magnetic resonance imaging. We aimed to compare diffusion tensor imaging findings between inflammatory and neoplastic intramedullary spinal cord lesions, with a specific focus on patterns of fiber tracking.
MATERIALS AND METHODS
Diffusion tensor imaging was performed in patients with either inflammatory or neoplastic intramedullary spinal cord lesions. The fiber tracking patterns (categorized as "intact,""displaced," or "interrupted") were compared between these two groups.
RESULTS
Eight patients were included in the study: 5 patients with pathologically or clinically confirmed inflammatory lesions and 3 patients with pathologically or clinically confirmed neoplastic lesions. Among the 5 patients with inflammatory lesions, 2 patients exhibited the displaced pattern and 3 patients exhibited the intact pattern. Among the 3 patients with neoplastic lesions, 1 patient exhibited the intact pattern, 1 patient exhibited the displaced pattern, and 1 patient exhibited the interrupted pattern.
CONCLUSION
In this study, inflammatory and neoplastic intramedullary spinal cord lesions were not clearly differentiated by fiber tracking; both conditions can present with overlapping features such as displaced fibers. The exclusion of inflammatory conditions based on the presence of displaced fibers in fiber tracking images should be avoided.
MeSH Terms
Figure
-
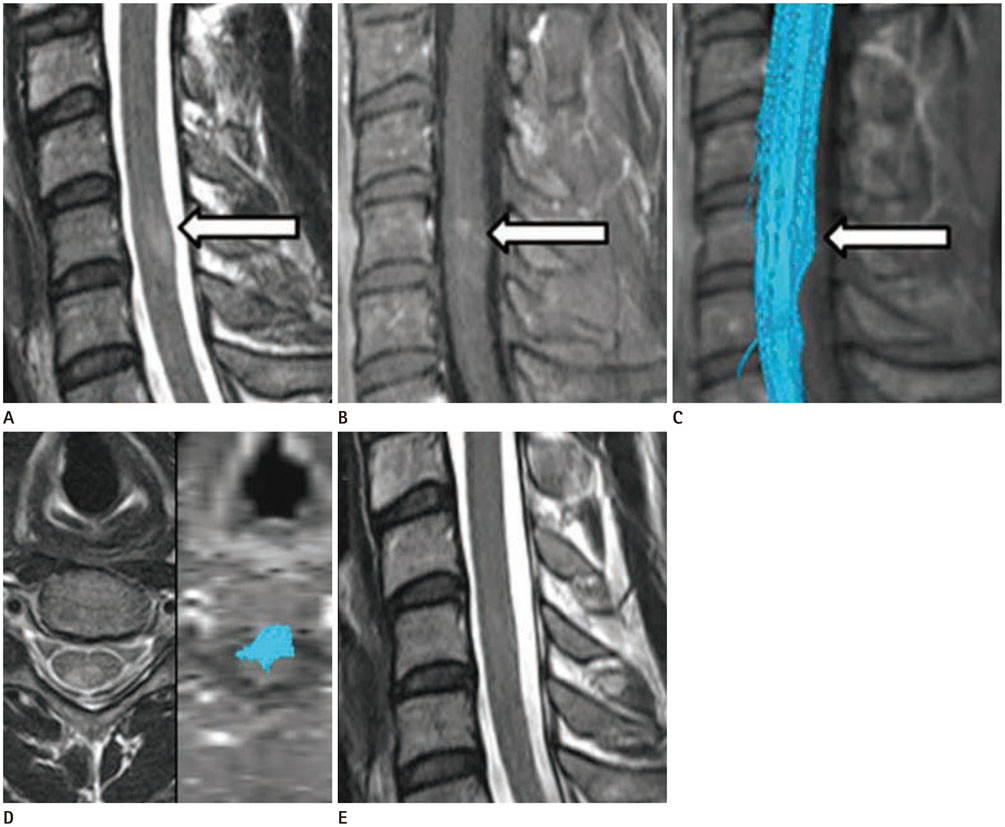
Fig. 1 A 34-year-old man with a tingling sensation throughout the whole body, who was clinically confirmed as having an inflammatory intramedullary spinal cord lesion (case number 3). A. An intramedullary lesion is located at the C5 level of the spinal cord on T2-weighted imaging (white arrow). B. The lesion shows enhancement (white arrow). C. On FT, the fibers appear intact without displacement or interruption (white arrow). D. FT image is mis-registered anteriorly. E. After 4 months of steroid therapy, no lesion or symptom is noted. FT = fiber tracking

Fig. 2 A 52-year-old woman with sudden-onset progressive left side weakness and binocular diplopia, who was clinically confirmed as having an inflammatory intramedullary spinal cord lesion (case number 5). A. An intramedullary lesion is located at the C2 to C5 level of the spinal cord on T2-weighted imaging. B. The lesion shows focal enhancement. C. FT of the lesion shows bilaterally displaced fibers. D. After 5 months of steroid pulse therapy, a decreased extent of enhancement is noted on contrast-enhanced T1-weighted imaging. FT = fiber tracking
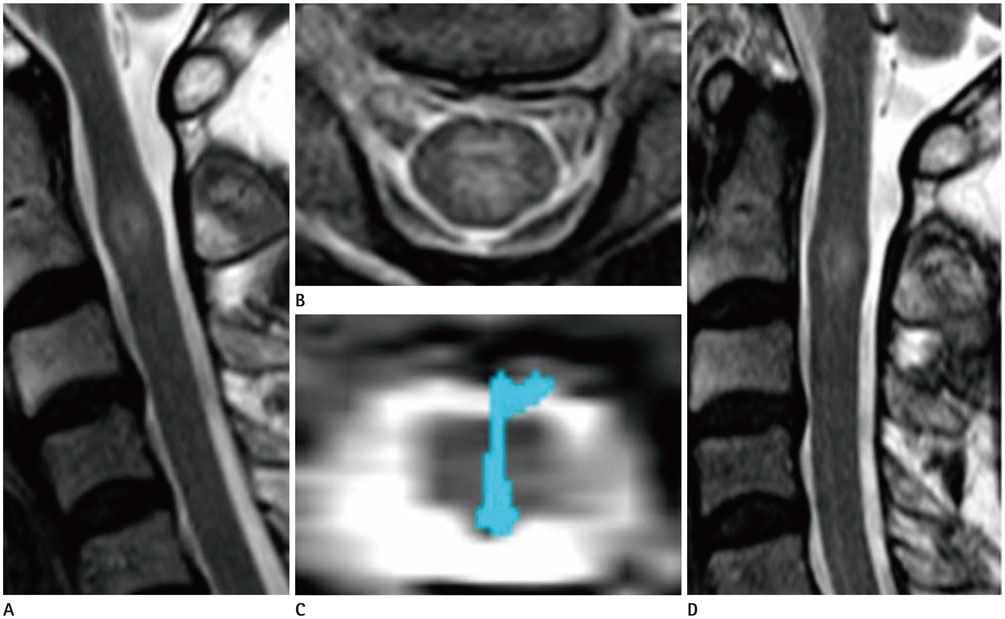
Fig. 3 A 54-year-old woman with pain in both shoulders, who was clinically confirmed as having a neoplastic intramedullary spinal cord lesion (case number 6). A. An intramedullary lesion is located at the C2 level of the spinal cord on T2-weighted imaging. B. The axial plane of the lesion on T2-weighted imaging. C. FT shows intact fibers. D. After 1 year, a stable lesion is observed on follow-up magnetic resonance imaging. FT = fiber tracking
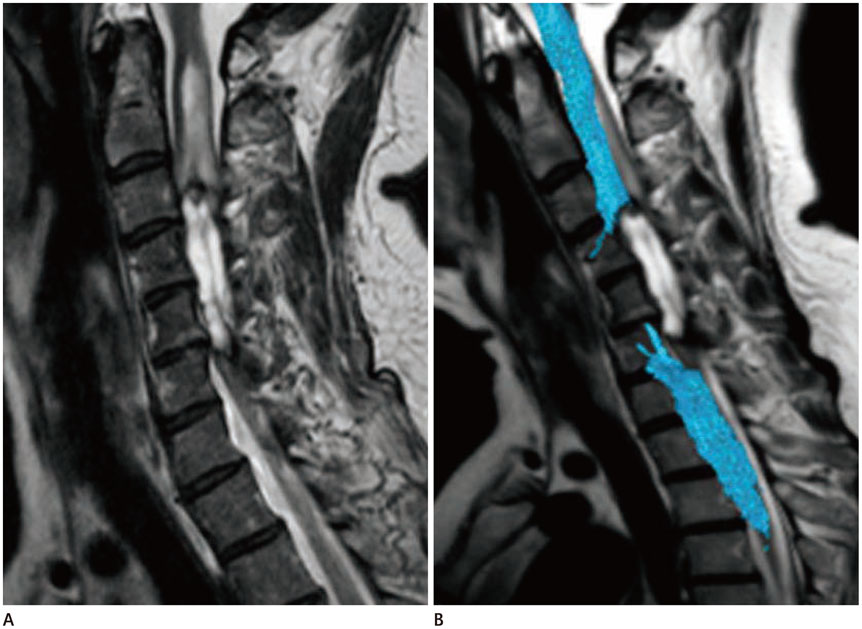
Fig. 4 A 55-year-old woman with paresthesia in both arms, who was pathologically confirmed as having an ependymoma (case number 7). A. A cystic lesion is located from the C3 to C5/6 level of the spinal cord on T2-weighted imaging. B. FT shows interrupted fibers. FT = fiber tracking
Reference
-
1. Brinar M, Rados M, Habek M, Poser CM. Enlargement of the spinal cord: inflammation or neoplasm? Clin Neurol Neurosurg. 2006; 108:284–289.2. Habek M, Adamec I, Brinar VV. Spinal cord tumor versus transverse myelitis. Spine J. 2011; 11:1143–1145.3. El Maati AAA, Chalabi N. Diffusion tensor tractography as a supplementary tool to conventional MRI for evaluating patients with myelopathy. Egypt J Radiol Nucl Med. 2014; 45:1223–1231.4. Thurnher MM, Law M. Diffusion-weighted imaging, diffusion-tensor imaging, and fiber tractography of the spinal cord. Magn Reson Imaging Clin N Am. 2009; 17:225–244.5. Werring DJ, Clark CA, Barker GJ, Thompson AJ, Miller DH. Diffusion tensor imaging of lesions and normal-appearing white matter in multiple sclerosis. Neurology. 1999; 52:1626–1632.6. Lee JW, Kim JH, Park JB, Park KW, Yeom JS, Lee GY, et al. Diffusion tensor imaging and fiber tractography in cervical compressive myelopathy: preliminary results. Skeletal Radiol. 2011; 40:1543–1551.7. Mori S, van Zijl PC. Fiber tracking: principles and strategies - a technical review. NMR Biomed. 2002; 15:468–480.8. Nimsky C. Fiber tracking--we should move beyond diffusion tensor imaging. World Neurosurg. 2014; 82:35–36.9. Clark CA, Werring DJ. Diffusion tensor imaging in spinal cord: methods and applications - a review. NMR Biomed. 2002; 15:578–586.10. Lerner A, Mogensen MA, Kim PE, Shiroisi MS, Hwang DH, Law M. Clinical applications of diffusion tensor imaging. World Neurosurg. 2014; 82:96–109.11. Lee JW, Park KS, Kim JH, Choi JY, Hong SH, Park SH, et al. Diffusion tensor imaging in idiopathic acute transverse myelitis. AJR Am J Roentgenol. 2008; 191:W52–W57.12. Facon D, Ozanne A, Fillard P, Lepeintre JF, Tournoux-Facon C, Ducreux D. MR diffusion tensor imaging and fiber tracking in spinal cord compression. AJNR Am J Neuroradiol. 2005; 26:1587–1594.13. Mamata H, Jolesz FA, Maier SE. Apparent diffusion coefficient and fractional anisotropy in spinal cord: age and cervical spondylosis-related changes. J Magn Reson Imaging. 2005; 22:38–43.14. Rajasekaran S, Kanna RM, Karunanithi R, Shetty AP. Diffusion tensor tractography demonstration of partially injured spinal cord tracts in a patient with posttraumatic Brown Sequard syndrome. J Magn Reson Imaging. 2010; 32:978–981.15. Ducreux D, Lepeintre JF, Fillard P, Loureiro C, Tadié M, Lasjaunias P. MR diffusion tensor imaging and fiber tracking in 5 spinal cord astrocytomas. AJNR Am J Neuroradiol. 2006; 27:214–216.16. Liu X, Tian W, Kolar B, Hu R, Huang Y, Huang J, et al. Advanced MR diffusion tensor imaging and perfusion weighted imaging of intramedullary tumors and tumor like lesions in the cervicomedullary junction region and the cervical spinal cord. J Neurooncol. 2014; 116:559–566.17. Setzer M, Murtagh RD, Murtagh FR, Eleraky M, Jain S, Marquardt G, et al. Diffusion tensor imaging tractography in patients with intramedullary tumors: comparison with intraoperative findings and value for prediction of tumor resectability. J Neurosurg Spine. 2010; 13:371–380.18. Giussani C, Poliakov A, Ferri RT, Plawner LL, Browd SR, Shaw DW, et al. DTI fiber tracking to differentiate demyelinating diseases from diffuse brain stem glioma. Neuroimage. 2010; 52:217–223.19. Vargas MI, Delavelle J, Jlassi H, Rilliet B, Viallon M, Becker CD, et al. Clinical applications of diffusion tensor tractography of the spinal cord. Neuroradiology. 2008; 50:25–29.20. Renoux J, Facon D, Fillard P, Huynh I, Lasjaunias P, Ducreux D, et al. MR diffusion tensor imaging and fiber tracking in inflammatory diseases of the spinal cord. AJNR Am J Neuroradiol. 2006; 27:1947–1951.21. Stadlbauer A, Buchfelder M, Salomonowitz E, Ganslandt O. Fiber density mapping of gliomas: histopathologic evaluation of a diffusion-tensor imaging data processing method. Radiology. 2010; 257:846–853.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anisotropy Measurement and Fiber Tracking of the White Matter by Using Diffusion Tensor MR Imaging: Influence of the Number of Diffusion-Sensitizing Gradient Direction
- Diffusion Metrics as a Potential Prognostic Biomarker in Cervical Myelopathy
- Diffusion Tensor Imaging and Cerebrospinal Fluid Flow Study of Cine Phase Contrast in Normal Cervical Spinal Cords
- Brain Diffusion Tensor MR Imaging
- High-Resolution Diffusion Tensor MR Imaging for Evaluating Myocardial Anisotropy and Fiber Tracking at 3T: the Effect of the Number of Diffusion-Sensitizing Gradient Directions
