Association of Bone Mineral Density with Airway Obstruction and Emphysema
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Ewha Medical Research Institute, Ewha Womans University School of Medicine, Seoul, Korea. jinhwalee@ewha.ac.kr
- 2Department of Radiology, Ewha Medical Research Institute, Ewha Womans University School of Medicine, Seoul, Korea.
Abstract
- BACKGROUND
Airway obstruction and the extent of emphysema are reported to be responsible for reduced bone mineral density (BMD). Corresponding to different phenotypes of a pulmonary disease, different severity in extra pulmonary features may exist. We compared BMDs of subjects with or without airway obstruction and/or emphysema and investigated the relationships among BMD, the severity of airway obstruction, and the extent of emphysema.
METHODS
Using a university hospital database, we reviewed patients over 40 years old who performed spirometry, computed tomography of chest, and measurement of BMD of the lumbar (L) spine. According to the presence or absence of airway obstruction and/or emphysema, four groups were classified.
RESULTS
Among a total of 59 subjects, 33 (56%) had osteoporosis. The prevalence of osteoporosis in subjects with no airway obstruction and no emphysema, those with only emphysema, those with only airway obstruction, and those with both airway obstruction and emphysema were 42%, 57%, 64%, and 73%, respectively (p=0.047 by linear-by-linear association). The mean T-scores of BMD of L1 (p=0.032) and L1-4 spines were different among the four groups (p=0.034). Although the T-score of L1 BMD negatively correlated with the extent of emphysema (r=-0.275, p=0.035) and positively with each of body mass index (BMI) (r=0.520, p<0.001), forced expiratory volume in one second (FEV1) (r=0.330, p=0.011), FEV1/forced vital capacity (r=0.409, p=0.001), and forced expiratory flow at 25~75% of FVC (FEF(25-75%)) (r=0.438, p=0.0001), respectively, multiple linear regression analysis indicated that BMI (p<0.001) and FEF(25-75%) were predictive of BMD (p=0.012).
CONCLUSION
Low BMI and airway obstruction were strongly associated with reduced bone density rather than the extent of emphysema.
MeSH Terms
Figure
-

Figure 1 Four groups of patients disclosed by the presence or absence of airway obstruction and/or emphysema. Group 1 (n=26) with no airway obstruction (AO) and no emphysema are presented as hollow circles; group 2 (n=7) with emphysema and no AO, full circles; group 3 (n=11) with AO and no emphysema, hollow triangles; and group 4 (n=15) with both AO and emphysema, full triangles.
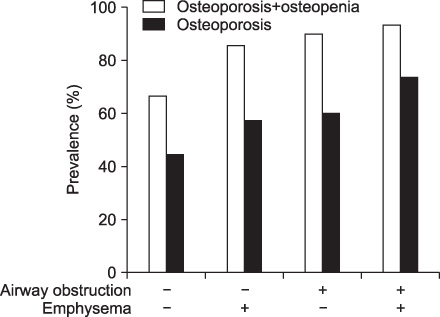
Figure 2 Association between the presence of reduced bone mineral density (BMD) and four groups. The prevalence of reduced BMD, including osteopenia and osteoporosis, and osteoporosis in the four groups were: 65%, 86%, 91%, and 93% (p=0.021 linear-by-linear association) and 42%, 57%, 64%, and 73% (p=0.047 linear-by-linear association), respectively.
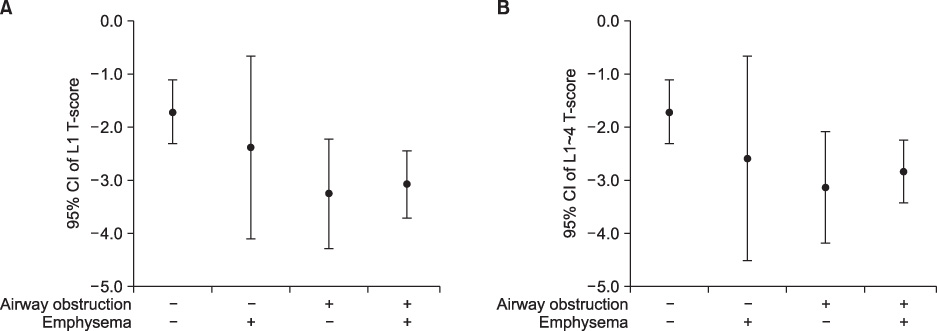
Figure 3 (A, B) T-scores of L1 and L1~4 in four groups. CI: confidence interval.
Reference
-
1. Iqbal F, Michaelson J, Thaler L, Rubin J, Roman J, Nanes MS. Declining bone mass in men with chronic pulmonary disease: contribution of glucocorticoid treatment, body mass index, and gonadal function. Chest. 1999. 116:1616–1624.2. Katsura H, Kida K. A comparison of bone mineral density in elderly female patients with COPD and bronchial asthma. Chest. 2002. 122:1949–1955.3. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009. 33:1165–1185.4. Bolton CE, Cannings-John R, Edwards PH, Ionescu AA, Evans WD, Pettit RJ, et al. What community measurements can be used to predict bone disease in patients with COPD? Respir Med. 2008. 102:651–657.5. Bon J, Fuhrman CR, Weissfeld JL, Duncan SR, Branch RA, Chang CC, et al. Radiographic emphysema predicts low bone mineral density in a tobacco-exposed cohort. Am J Respir Crit Care Med. 2011. 183:885–890.6. Incalzi RA, Caradonna P, Ranieri P, Basso S, Fuso L, Pagano F, et al. Correlates of osteoporosis in chronic obstructive pulmonary disease. Respir Med. 2000. 94:1079–1084.7. Kjensli A, Mowinckel P, Ryg MS, Falch JA. Low bone mineral density is related to severity of chronic obstructive pulmonary disease. Bone. 2007. 40:493–497.8. Maggi S, Siviero P, Gonnelli S, Schiraldi C, Malavolta N, Nuti R, et al. Osteoporosis risk in patients with chronic obstructive pulmonary disease: the EOLO study. J Clin Densitom. 2009. 12:345–352.9. Ohara T, Hirai T, Muro S, Haruna A, Terada K, Kinose D, et al. Relationship between pulmonary emphysema and osteoporosis assessed by CT in patients with COPD. Chest. 2008. 134:1244–1249.10. Vrieze A, de Greef MH, Wijkstra PJ, Wempe JB. Low bone mineral density in COPD patients related to worse lung function, low weight and decreased fat-free mass. Osteoporos Int. 2007. 18:1197–1202.11. American Thoracic Society. Standardization of Spirometry, 1994 Update. Am J Respir Crit Care Med. 1995. 152:1107–1136.12. Hwang YI, Kim CH, Kang HR, Shin T, Park SM, Jang SH, et al. Comparison of the prevalence of chronic obstructive pulmonary disease diagnosed by lower limit of normal and fixed ratio criteria. J Korean Med Sci. 2009. 24:621–626.13. Swanney MP, Ruppel G, Enright PL, Pedersen OF, Crapo RO, Miller MR, et al. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Thorax. 2008. 63:1046–1051.14. Gevenois PA, de Maertelaer V, De Vuyst P, Zanen J, Yernault JC. Comparison of computed density and macroscopic morphometry in pulmonary emphysema. Am J Respir Crit Care Med. 1995. 152:653–657.15. Kanis JA, Melton LJ 3rd, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res. 1994. 9:1137–1141.16. Willemse BW, ten Hacken NH, Rutgers B, Lesman-Leegte IG, Postma DS, Timens W. Effect of 1-year smoking cessation on airway inflammation in COPD and asymptomatic smokers. Eur Respir J. 2005. 26:835–835.17. Shepherd AJ, Cass AR, Carlson CA, Ray L. Development and internal validation of the male osteoporosis risk estimation score. Ann Fam Med. 2007. 5:540–546.18. Balasubramanian VP, Varkey B. Chronic obstructive pulmonary disease: effects beyond the lungs. Curr Opin Pulm Med. 2006. 12:106–112.19. Eid AA, Ionescu AA, Nixon LS, Lewis-Jenkins V, Matthews SB, Griffiths TL, et al. Inflammatory response and body composition in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001. 164(8 Pt 1):1414–1418.20. Wouters EF. Local and systemic inflammation in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2005. 2:26–33.21. Cavanagh PR, Licata AA, Rice AJ. Exercise and pharmacological countermeasures for bone loss during long-duration space flight. Gravit Space Biol Bull. 2005. 18:39–58.22. Van Vliet M, Spruit MA, Verleden G, Kasran A, Van Herck E, Pitta F, et al. Hypogonadism, quadriceps weakness, and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005. 172:1105–1111.23. McKarns SC, Smith CJ, Morton MJ, Payne VM, Davis DL, Stringer LW, et al. Correlation of hematologic markers of inflammation and lung function: a comparison of asymptomatic smokers and nonsmokers. Hum Exp Toxicol. 1996. 15:523–532.24. Rao R, Frederick JM, Enander I, Gregson RK, Warner JA, Warner JO. Airway function correlates with circulating eosinophil, but not mast cell, markers of inflammation in childhood asthma. Clin Exp Allergy. 1996. 26:789–793.25. Choi JW, Pai SH. Association between respiratory function and osteoporosis in pre- and postmenopausal women. Maturitas. 2004. 48:253–258.26. Lekamwasam S, Trivedi DP, Khaw KT. An association between respiratory function and bone mineral density in women from the general community: a cross sectional study. Osteoporos Int. 2002. 13:710–715.27. Lekamwasam S, Trivedi DP, Khaw KT. An association between respiratory function and hip bone mineral density in older men: a cross-sectional study. Osteoporos Int. 2005. 16:204–207.28. Gan WQ, Man SF, Sin DD. The interactions between cigarette smoking and reduced lung function on systemic inflammation. Chest. 2005. 127:558–564.29. Watz H, Waschki B, Boehme C, Claussen M, Meyer T, Magnussen H. Extrapulmonary effects of chronic obstructive pulmonary disease on physical activity: a cross-sectional study. Am J Respir Crit Care Med. 2008. 177:743–751.30. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005. 26:948–968.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Osteoporosis
- The relationship of maturation value of vaginal epithelium and bone mineral density in postmenopausal women
- Measurement of bone mineral density in Korean newborns by dual photon absorptiometry
- Change in bone mineral density according to aging in Korean women: Study of Using Quantitative Computerized Tomography
- The relationship between grip strength and femoral and vertebral bone mineral density in peri-and postmenopausal women
