Petrositis With Bilateral Abducens Nerve Palsies complicated by Acute Otitis Media
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. ashock@hanmail.net
Abstract
- Petrous apicitis is a rare but fatal complication of otitis media. An infection within the middle ear can extend within the temporal bone into the air cells of the petrous apex. With only the thin dura mater separating the trigeminal ganglion and the 6th cranial nerve from the bony petrous apex, they are vulnerable to inflammatory processes, resulting in deep facial pain, lateral rectus muscle paralysis, and diplopia. In 1904, Gradenigo described a triad of symptoms related to petrous apicitis, including acute suppurative otitis media, deep facial pain resulting from trigeminal involvement, and abducens nerve palsy. It has traditionally been treated with surgery, but recent advances in imaging, with improved antibiotic treatment, allow conservative management. In this case report, we describe a clinical and neuroradiological evolution of a child with a petrous apicitis after acute otitis media, which was managed medically with a positive outcome.
Keyword
MeSH Terms
Figure
-
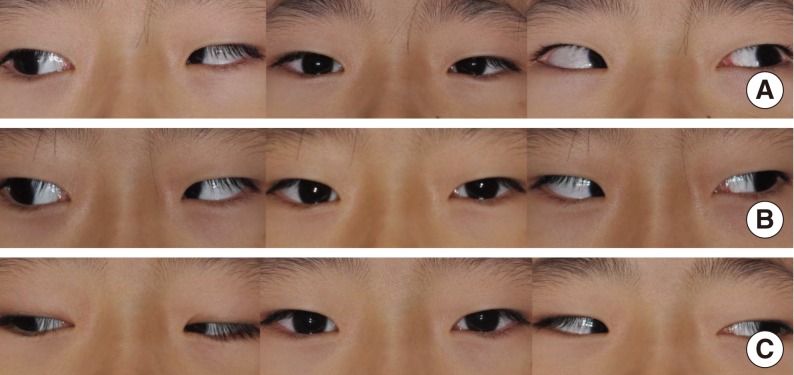
Fig. 1 Photography of the eyes at initial (A), the 16th hospital day (B), and the 30th hospital day (C). The patient had left strabismus at central gaze, and inability of full lateral gaze of both eyes suggesting both abducens nerve palsy at initial (A). Improvement of left strabismus at central gaze accompanying central diplopia and much improvement of lateral gaze of both eyes were shown at the16th hospital day (B). Improvement of left strabismus at central gaze without central diplopia, and further improvement of lateral gaze of both eyes were shown at the 30th hospital day (day of discharge).
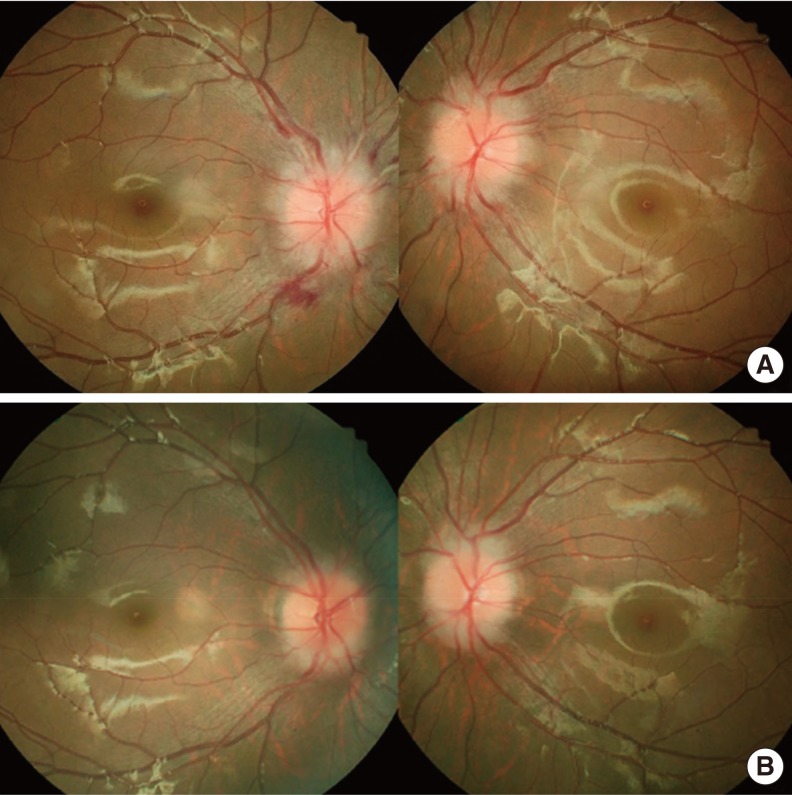
Fig. 2 Fundoscopic examinations at admission (A), and at six weeks after admission (B). There was severe swelling of bilateral optic discs at admission day (A), and much improvement of blurring of the optic disc margins after six weeks (B).
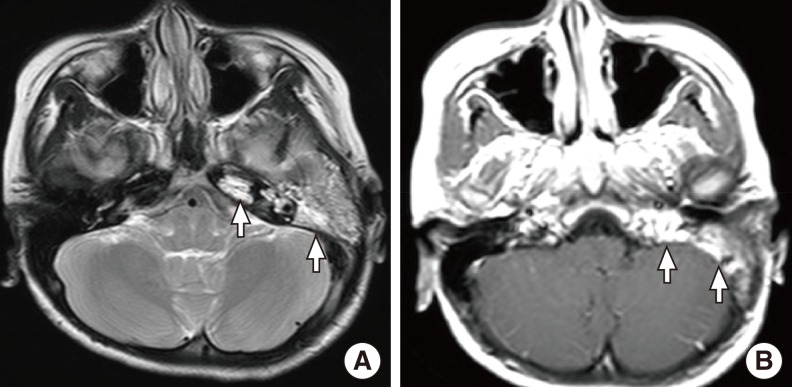
Fig. 3 Brain magnetic resonance imaging (MRI) findings at admission: T2 weighted MRI finding (A) and T1 weighted enhanced MRI finding (B). These showed high signal intensities involving left mastoid and petrous apex (arrows).
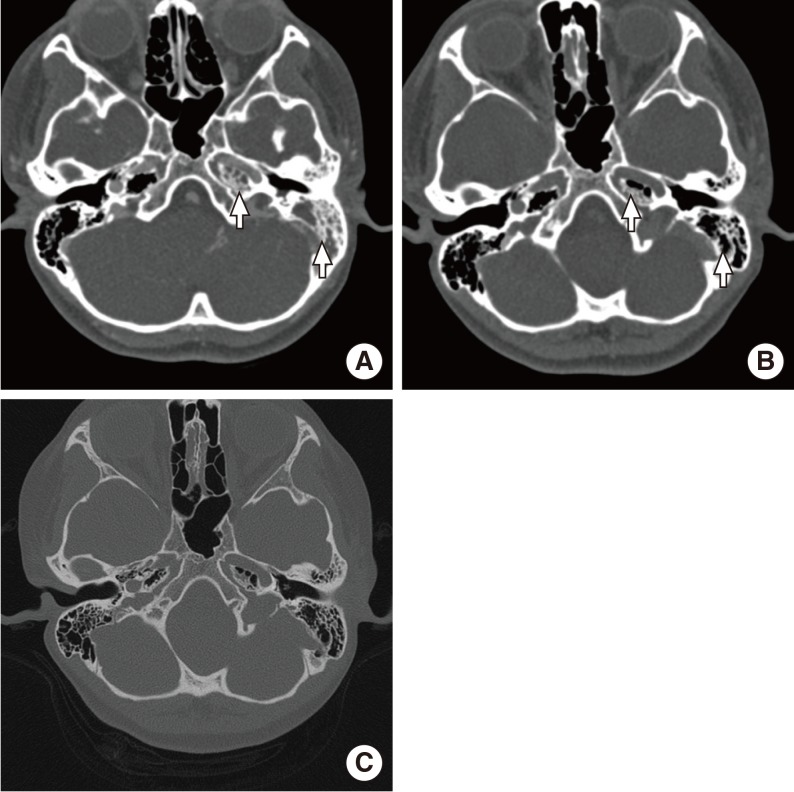
Fig. 4 Temporal bone computed tomography (CT) with contrast enhancement at the 9th hospital day, showing extended pneumatization of left temporal bone to petrous apex and soft tissue densities at left mastoid and petrous apex (A). At the 21th hospital day, improved aeration of left petrous apex and mastoid with some residual soft tissue densities are shown (B). Temporal bone CT at two weeks after discharge date, showing further improvement of aeration of left petrous apex and mastoid with ventilation tube in situ (C).
Reference
-
1. Chole RA, Sudhoff HH. Chronic otitis media, mastoiditis, and petrositis. In : Flint PW, Haughey BH, Lund VJ, Niparko JK, Richardson MA, Robbins KT, editors. Cummings otolaryngology head and neck surgery. 5th ed. Philadelphia, PA: Mosby;c2010. p. 1963–1978.2. El-Kashlan HK, Harker LA, Shelton C, Aygun N, Niparko JK. Complications of temporal bone infections. In : Flint PW, Haughey BH, Lund VJ, Niparko JK, Richardson MA, Robbins KT, editors. Cummings otolaryngology head and neck surgery. 5th ed. Philadelphia, PA: Mosby;c2010. p. 1979–1998.3. Burston BJ, Pretorius PM, Ramsden JD. Gradenigo's syndrome: successful conservative treatment in adult and paediatric patients. J Laryngol Otol. 2005; 4. 119(4):325–329. PMID: 15949093.
Article4. Lutter SA, Kerschner JE, Chusid MJ. Gradenigo syndrome: a rare but serious complication of otitis media. Pediatr Emerg Care. 2005; 6. 21(6):384–386. PMID: 15942518.5. Marianowski R, Rocton S, Ait-Amer JL, Morisseau-Durand MP, Manach Y. Conservative management of Gradenigo syndrome in a child. Int J Pediatr Otorhinolaryngol. 2001; 1. 57(1):79–83. PMID: 11165646.
Article6. Lee NH, Ban JH, Park CY, Kim CC. A case of petrositis with abducens palsy. Korean J Otolaryngol-Head Neck Surg. 2006; 8. 49(8):869–872.7. Shin HS, Yoo HK, Suh YR. A case of unusual petrositis. Korean J Otolaryngol-Head Neck Surg. 1964; 6. 7(2):59–62.8. Lee KC, Chio C, Park KY, Park MS. A case of Gradenigo's syndrome combining epidural abscess and Bezold's abscess. Korean J Otolaryngol-Head Neck Surg. 1989; 6. 32(3):567–571.9. Park SN, Yeo SW, Rhyoo JY, Lee HY. A case of cavernous sinus thrombophlebitis and abducence nerve palsy secondary to petrositis. Korean J Otolaryngol-Head Neck Surg. 2002; 1. 45(1):82–85.10. Goldstein NA, Casselbrant ML, Bluestone CD, Kurs-Lasky M. Intratemporal complications of acute otitis media in infants and children. Otolaryngol Head Neck Surg. 1998; 11. 119(5):444–454. PMID: 9807067.
Article11. Gillanders DA. Gradenigo's syndrome revisited. J Otolaryngol. 1983; 6. 12(3):169–174. PMID: 6876244.12. Sternberg I, Ronen S, Arnon N. Recurrent, isolated, post-febrile abducens nerve palsy. J Pediatr Ophthalmol Strabismus. 1980; Sep-Oct. 17(5):323–324. PMID: 7441445.
Article13. Laurens MB, Becker RM, Johnson JK, Wolf JS, Kotloff KL. MRSA with progression from otitis media and sphenoid sinusitis to clival osteomyelitis, pachymeningitis and abducens nerve palsy in an immunocompetent 10-year-old patient. Int J Pediatr Otorhinolaryngol. 2008; 7. 72(7):945–951. PMID: 18472169.
Article14. Peters GB 3rd, Bakri SJ, Krohel GB. Cause and prognosis of nontraumatic sixth nerve palsies in young adults. Ophthalmology. 2002; 10. 109(10):1925–1928. PMID: 12359616.
Article15. Chole RA, Donald PJ. Petrous apicitis: clinical considerations. Ann Otol Rhinol Laryngol. 1983; Nov-Dec. 92(6 Pt 1):544–551. PMID: 6660745.16. Watkyn-Thomas FW. The treatment of petrositis: (section of otology). Proc R Soc Med. 1936; 1. 29(3):267–274. PMID: 19990585.17. Hendershot EL, Wood JW, Bennhoff D. The middle cranial fossa approach to the petrous apex. Laryngoscope. 1976; 5. 86(5):658–663. PMID: 933655.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Petrositis with Abducens Palsy
- Abducens Nerve Palsy Complicated by Inferior Petrosal Sinus Septic Thrombosis Due to Mastoiditis
- Management of Otitis Media in Children
- Unilateral Abducens Nerve Palsy Associated with Ruptured Anterior Communicating Artery Aneurysm
- Delayed Bilateral Abducens Nerve Palsy after Head Trauma
