Unilateral Abducens Nerve Palsy Associated with Ruptured Anterior Communicating Artery Aneurysm
- Affiliations
-
- 1Department of Neurosurgery, Gil Hospital, Gachon University of Medicine and Science, Incheon, Korea. cwpark@gilhospital.com
- KMID: 1427729
- DOI: http://doi.org/10.13004/kjnt.2012.8.2.146
Abstract
- Isolated unilateral abducens nerve palsies associated with spontaneous subarachnoid hemorrhage have rarely been reported, and their association with anterior communicating artery is even rarer. We report two cases of unilateral abducens nerve palsies following rupture of anterior communicating artery aneurysms. The aneurysms were successfully clipped, and abducens nerve palsies were gradually recovered.
MeSH Terms
Figure
-
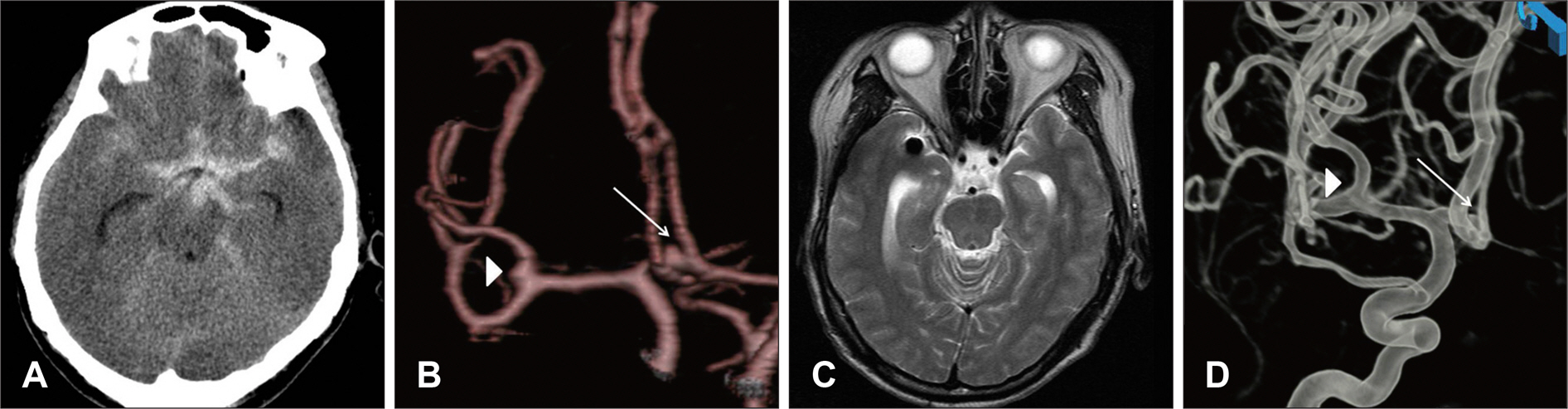
FIGURE 1. Radiological findings of case 1. A: Head computed tomography (CT) showing subarachnoid hemorrhage of Fisher's grade 3. B: Cerebral CT angiography. Arrows indicate anterior communicating artery and arrow head middle cerebral artery aneurysms, respectively. C: Brain magnetic resonance image demonstrating no definitive abnormal lesion in the brain stem. D: Postoperative cerebral angiography indicating complete disappearance of aneurysms and no vascular abnormality.
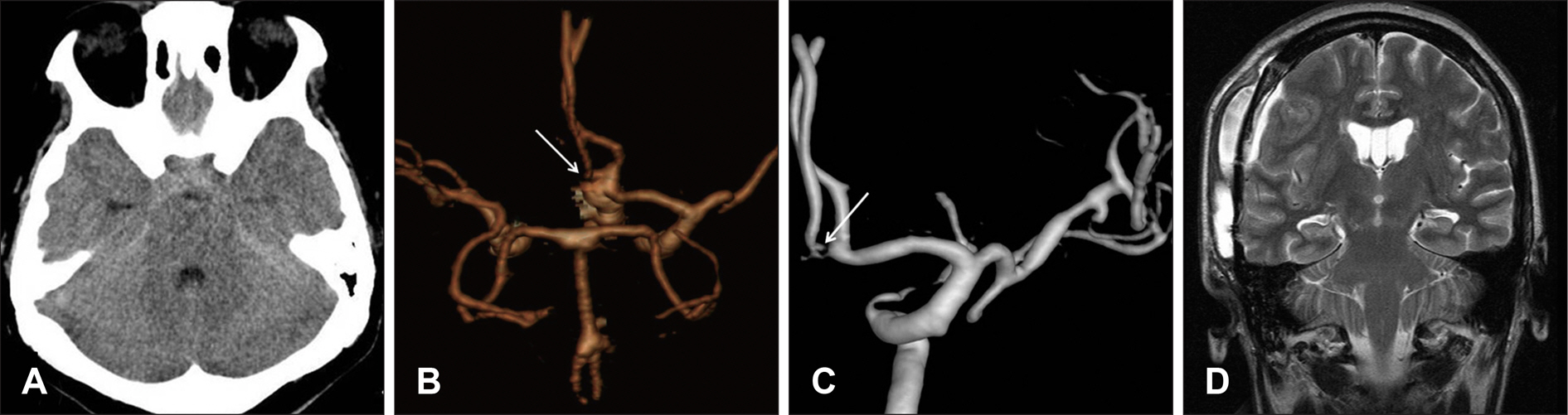
FIGURE 2. Radiological findings of case 2. A: Head computed tomography (CT) showing subarachnoid hemorrhage of Fisher's grade 2. B: Cerebral CT angiography. Arrow indicates anterior communicating artery aneurysm. C: Postoperative cerebral angiography indicating no residual aneurysmal sac or vascular abnormality. D: Brain magnetic resonance image demonstrating a small amount of fluid collection over the right frontotemporal convexity with unremarkable brain stem area.
Reference
-
1). Akagi T., Miyamoto K., Kashii S., Yoshimura N. Cause and prognosis of neurologically isolated third, fourth, or sixth cranial nerve dysfunction in cases of oculomotor palsy. Jpn J Ophthalmol. 52:32–35. 2008.
Article2). Berlit P. Isolated and combined pareses of cranial nerves III, IV and VI. A retrospective study of 412 patients. J Neurol Sci. 103:10–15. 1991.
Article3). Collins TE., Mehalic TF., White TK., Pezzuti RT. Trochlear nerve palsy as the sole initial sign of an aneurysm of the superior cerebellar artery. Neurosurgery. 30:258–261. 1992.
Article4). Laun A., Tonn JC. Cranial nerve lesions following subarachnoid hemorrhage and aneurysm of the circle of Willis. Neurosurg Rev. 11:137–141. 1988.
Article5). Nathal E., Yasui N., Suzuki A., Hadeishi H. Ruptured anterior communicating artery aneurysm causing bilateral abducens nerve paralyses—case report. Neurol Med Chir (Tokyo). 32:17–20. 1992.6). Plum F., Posner JB. The diagnosis of stupor and coma, ed 3. Philadelphia: F. A. Davis Company, pp113-114. 1980.7). Rush JA., Younge BR. Paralysis of cranial nerves III, IV, and VI. Cause and prognosis in 1,000 cases. Arch Ophthalmol. 99:76–79. 1981.8). Suzuki J., Iwabuchi T. Ocular motor disturbances occurring as false localizing signs in ruptured intracranial aneurysms. Acta Neurochir (Wien). 30:119–128. 1974.
Article9). Ziyal IM., Ozcan OE., Deniz E., Bozkurt G., Ismailoğlu O. Early improvement of bilateral abducens nerve palsies following surgery of an anterior communicating artery aneurysm. Acta Neurochir (Wien). 145:159–161. discussion 161. 2003.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Slowly Recovering Isolated Bilateral Abducens Nerve Palsy after Embolization of Ruptured Anterior Communicating Artery Aneurysm
- Ruptured Posterior Communicating Artery Aneurysm Causing Bilateral Abducens Nerve Paralyses: Case Report
- Ruptured Anterior Communicating Artery Aneurysm Causing Bilateral Oculomotor Nerve Palsy: A Case Report
- Isolated, Contralateral Trochlear Nerve Palsy Associated with a Ruptured Right Posterior Communicating Artery Aneurysm
- Isolated Bilateral Abducens Nerve Palsy Caused by Basilar Artery Dissecting Aneurysm
