Abducens Nerve Palsy Complicated by Inferior Petrosal Sinus Septic Thrombosis Due to Mastoiditis
- Affiliations
-
- 1Department of Ophthalmology, Maryknoll Hospital, Busan, Korea.
- 2Department of Otorhinolaryngology, Maryknoll Hospital, Busan, Korea.
- 3Department of Ophthalmology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. kris9352@hanmail.net
- KMID: 1120186
- DOI: http://doi.org/10.3341/kjo.2012.26.1.65
Abstract
- We present a very rare case of a 29-month-old boy with acute onset right abducens nerve palsy complicated by inferior petrosal sinus septic thrombosis due to mastoiditis without petrous apicitis. Four months after mastoidectomy, the patient fully recovered from an esotropia of 30 prism diopters and an abduction limitation (-4) in his right eye.
MeSH Terms
Figure
-
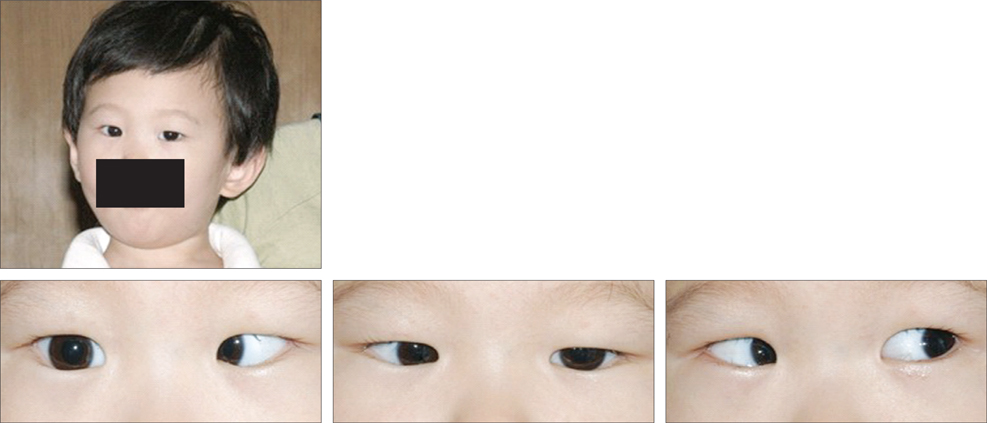
Fig. 1 Photographs show an anomalous head posture of right-turning facial position, an abduction defect (-4), and an esodeviation of 30 prism diopters in his right eye. Informed consent was received from parents of the patient.
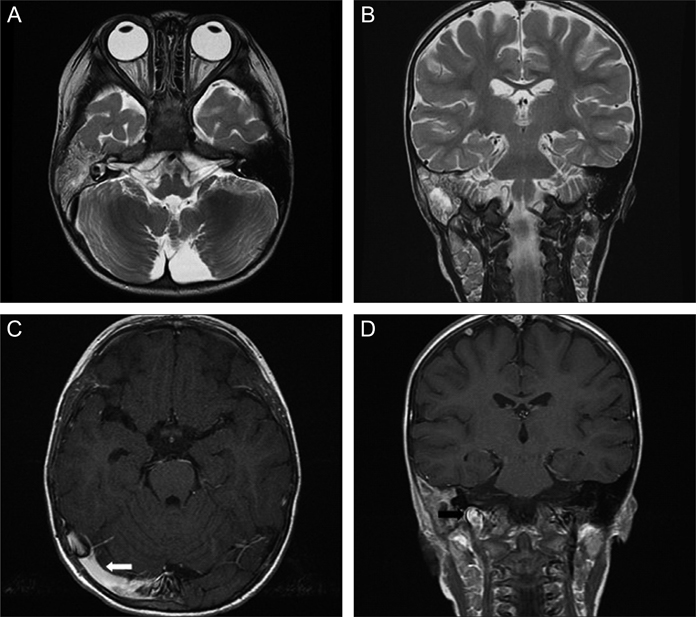
Fig. 2 (A) Preoperative axial enhanced T2-weighted magnetic resonance (MR) image shows right otomastoiditis. (B) Preoperative coronal enhanced T2-weighted MR image shows right otomastoiditis. (C) Axial enhanced T1-weighted MR image shows slow flow velocity of the right transverse sinus (white arrow). (D) Coronal enhanced T1-weighted MR image shows slow-flow velocity of the right internal jugular vein (black arrow).

Fig. 3 Computed tomography of the right temporal bone shows no inflammation of the petrous bone (white arrow) and an erosive mastoid septa (black arrow).

Fig. 4 Photographs show orthotropia and no limitation of abduction in the right eye at 4 months after mastoidectomy.
Reference
-
1. Sherman SC, Buchanan A. Gradenigo syndrome: a case report and review of a rare complication of otitis media. J Emerg Med. 2004. 27:253–256.2. Laurens MB, Becker RM, Johnson JK, et al. MRSA with progression from otitis media and sphenoid sinusitis to clival osteomyelitis, pachymeningitis and abducens nerve palsy in an immunocompetent 10-year-old patient. Int J Pediatr Otorhinolaryngol. 2008. 72:945–951.3. Homer JJ, Johnson IJ, Jones NS. Middle ear infection and sixth nerve palsy. J Laryngol Otol. 1996. 110:872–874.4. Ludman H, editor. Mawson's disease of the ear. 1988. 5th ed. London: Edward Arnold;479–536.5. Knox DL, Clark DB, Schuster FF. Benign VI nerve palsies in children. Pediatrics. 1967. 40:560–564.6. Goodwin D. Differential diagnosis and management of acquired sixth cranial nerve palsy. Optometry. 2006. 77:534–539.7. Kim BS, Do HM, Marks MP. Diagnosis and management of cerebral venous and sinus thrombosis. Semin Cerebrovasc Dis Stroke. 2004. 4:205–216.8. Biousse V, Newman NJ. Venous disease of the central nervous system. Semin Cerebrovasc Dis Stroke. 2004. 4:2–17.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Abducens Nerve Palsy due to a Dural Arteriovenous Fistula with Drainage into the Inferior Petrosal Sinus
- A Case of Raymond-Cestan Syndrome Caused by Inferior Petrosal Sinus Sampling
- Oculomotor and Abducens Nerve Palsy Complicated by Cavernous Sinus Thrombophlebitis Resulting from Acute Sinusitis
- Reversible Abducens Nerve Palsy Following Transvenous Embolization of Cavernous Sinus Dural Arteriovenous Fistula
- A Case of Cavernous Sinus Thrombophlebitis and Abducence Nerve Palsy Secondary to Petrositis
