A Case of Gossypiboma Masquerading as a Gastrointestinal Stromal Tumor
- Affiliations
-
- 1Department of Internal Medicine, Catholic University of Daegu College of Medicine, Daegu, Korea. kimey@cu.ac.kr
- 2Department of Surgery, Catholic University of Daegu College of Medicine, Daegu, Korea.
Abstract
- Gossypiboma refers to a mass resulting from a retained gauze pad accidentally left within the body after surgery. Although the clinical features are diverse, it is often found incidentally as a mass having an internal cystic change and adhesion to adjacent organs. Abdominal computed tomography (CT) is helpful, yet the initial diagnosis can be misleading in cases with atypical findings. We report a case of gossypiboma in a 78-year-old woman that we suspected was a gastrointestinal stromal tumor according to abdominal CT and endoscopic ultrasound, yet was diagnosed as a gossypiboma postoperatively.
Figure
-

Fig. 1 Abdominal computed tomography finding. A well-circumscribed, 5.5 cm-sized round mass with irregular internal calcification is noted in contiguity with the gastric fundus.
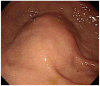
Fig. 2 EGD finding. A bulging lesion with normal overlying mucosa was seen at the fundus.

Fig. 3 Endoscopic ultrasonography findings. (A) An exophytic growing hypoechoic mass showing central linear hyperechoic area with posterior acoustic shadowing was noted. (B) Hypoechoic mass with internal irregular hyperechoic spots. (C) The mass is connected with fourth gastric wall layer and gastric serosal layer was not delineated.

Fig. 4 Gross findings. The mass is found to be a retained surgical sponge, so-called 'gossypiboma' surrounded by inflammatory pseudomembranous tissue which is tightly attached to gastric wall.
Reference
-
1. Lu YY, Cheung YC, Ko SF, Ng SH. Calcified reticulate rind sign: a characteristic feature of gossypiboma on computed tomography. World J Gastroenterol. 2005; 11:4927–4929. PMID: 16097075.
Article2. Yamamura N, Nakajima K, Takahashi T, et al. Intra-abdominal textiloma. A retained surgical sponge mimicking a gastric gastrointestinal stromal tumor: report of a case. Surg Today. 2008; 38:552–554. PMID: 18516538.
Article3. Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med. 2003; 348:229–235. PMID: 12529464.
Article4. Sturdy JH, Baird RM, Gerein AN. Surgical sponges: a cause of granuloma and adhesion formation. Ann Surg. 1967; 165:128–134. PMID: 6066852.5. Choi BI, Kim SH, Yu ES, Chung HS, Han MC, Kim CW. Retained surgical sponge: diagnosis with CT and sonography. AJR Am J Roentgenol. 1988; 150:1047–1050. PMID: 3282401.
Article6. Kokubo T, Itai Y, Ohtomo K, Yoshikawa K, Iio M, Atomi Y. Retained surgical sponges: CT and US appearance. Radiology. 1987; 165:415–418. PMID: 3310095.
Article7. Kopka L, Fischer U, Gross AJ, Funke M, Oestmann JW, Grabbe E. CT of retained surgical sponges (textilomas): pitfalls in detection and evaluation. J Comput Assist Tomogr. 1996; 20:919–923. PMID: 8933791.
Article8. Kwon JG, Kim EY, Kim YS, et al. Accuracy of endoscopic ultrasonographic impression compared with pathologic diagnosis in gastrointestinal submucosal tumors. Korean J Gastroenterol. 2005; 45:88–96. PMID: 15725712.9. Kim EY. Endoscopic ultrasonography in locoregional staging of gastric cancer. Korean J Gastroenterol. 2008; 52:124–127. PMID: 19077506.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of huge Gastrointestinal stromal tumor masquerading as an ovarian malignancy
- Intracranial Gossypiboma Mimicking a Recurrent Low Grade Astrocytoma: Case Report
- A Case of Massive Bleeding from Jejunal Stromal Tumor Diagnosed by Intraoperative Enteroscopy: A Case of Jejunal Stromal Tumor Bleeding
- A Case of Epithelioid Type Gastric Gastrointestinal Stromal Tumor with Gastrointestinal Bleeding
- Gastrointestinal Stromal Tumor of the Appendix Mimicking a Mucinous Cystadenocarcinoma: A Case Report
