Intracranial Gossypiboma Mimicking a Recurrent Low Grade Astrocytoma: Case Report
- Affiliations
-
- 1Department of Radiology, Dongguk University Il-San Hospital, Goyang, Korea. koojb@paran.com
- KMID: 2097940
- DOI: http://doi.org/10.3348/jksr.2011.64.3.217
Abstract
- Gossypiboma is an inflammatory pseudomass formed by a retained surgical sponge or gauze with reactive tissue after surgery. Gossypiboma has been reported most frequently after abdominal or thoracic surgery. As such, gossypiboma following brain surgery is very rare. We report a case of gossypiboma mimicking tumor recurrence in the brain after a craniotomy and surgical excision of a low grade astrocytoma.
MeSH Terms
Figure
-
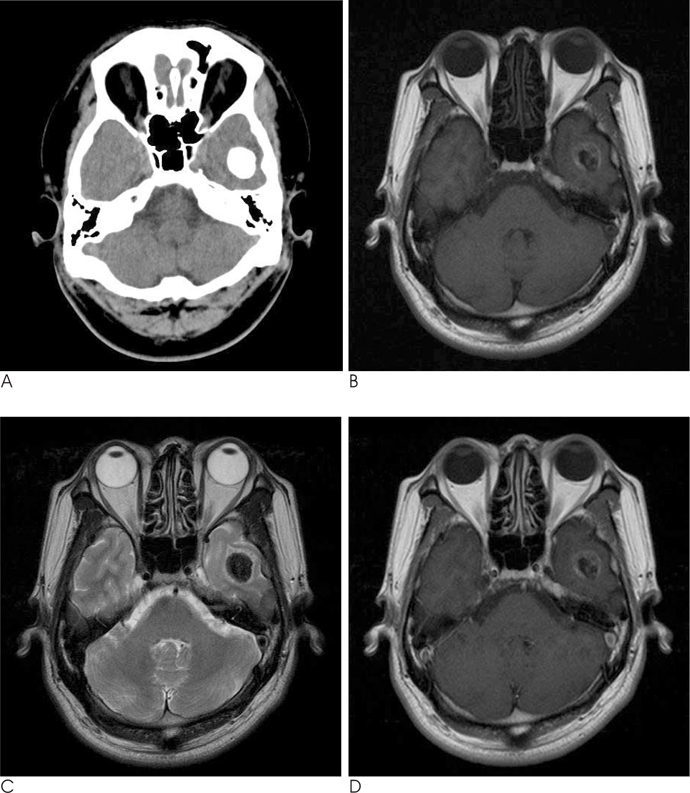
Fig. 1 CT and MR imaging show low grade astrocytoma in left temporal lobe. A. CT axial scan shows 2 × 2 cm ovoid dense calcified mass in left temporal lobe. B. T1-weighted axial image shows low signal intensity mass in left temporal lobe. C. T2-weighted axial image shows low signal intensity mass in left temporal lobe with minimal peritumoral edema. D. Contrast enhanced T1-weighted axial image shows no definite enhancement in mass.
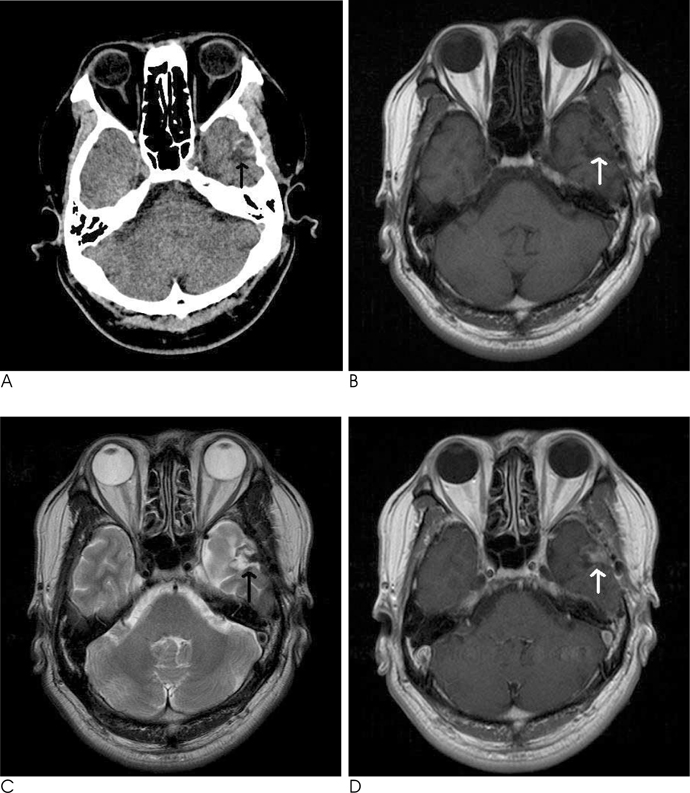
Fig. 2 After 6 months of the operation, the follow up CT and MR show intracranial gossypiboma mimicking recurrent low grade astrocytoma. A. CT axial scan shows 1 × 1.4 cm irregular heterogeneous slightly high density mass (arrow) in previous tumor resection site of left temporal lobe. B. T1-weighted axial image shows irregular shaped iso signal intensity mass (arrow) in left temporal lobe. C. T2-weighted axial image shows irregular shaped low signal intensity mass (arrow) in left temporal lobe. D. Contrast enhanced T1-weighted axial image shows relatively homogeneous enhancement in mass (arrow) in left temporal lobe.

Fig. 3 Microscopic finding shows intracranial gossypiboma. A. The low-power magnification shows a well-defined foreign body reaction within the brain parenchyme (×40). B. Higher magnification reveals multinucleated giant cells engulfing foreign body material surrounded by interstitial fibrosis and inflammation (× 200).
Reference
-
1. Rajput A, Loud PA, Gibbs JF, Kraybill WG. Diagnostic challenges in patients with tumors: case 1. Gossypiboma(foreign body) manifesting 30 years after laparotomy. J Clin Oncol. 2003; 21:3700–3701.2. Erdem G, Ates O, Koçak A, Alkan A. Lumbar gossypiboma Diagn. Diagn Interv Radiol. 2010; 16:10–12.3. Jang SW, Kim SJ, Kim SM, Lee JH, Choi CG, Lee DH, et al. MR spectroscopy and perfusion MR imaging findings of intracranial foreign body granuloma: a case report. Korean J Radiol. 2010; 11:359–363.4. Kim AK, Lee EB, Bagley LJ, Loevner LA. Retained surgical sponges after craniotomies: imaging appearances and complications. AJNR Am J Neuroradiol. 2009; 30:1270–1272.5. Martins MCB, Amaral RPG, Andrade CS, Lucato LT, Leite CC. Magnetic resonance imaging findings of intracranial gossypiboma: a case report and literature review. Radiol Bras. 2009; 42:407–409.6. Kopka L, Fischer U, Gross AJ, Funke M, Oestmann JW, Grabbe E. CT of retained surgical sponges (textilomas): pitfalls in detection and evaluation. J Comput Assist Tomogr. 1996; 20:919–923.7. Choi BI, Kim SH, Yu ES, Chung HS, Han MC, Kim CW. Retained surgical sponge: diagnosis with CT and sonography. AJR Am J Roentgenol. 1988; 150:1047–1050.8. Djindjian M, Brugieres P, Razavi-Encha F, Allegret C, Poirier J. Post-operative intracranial foreign body granuloma: a case report. Neuroradiology. 1987; 29:497–499.9. Chater-Cure G, Fonnegra-Caballero A, Baldión-Elorza AM, Jiménez-Hakim . Gossypiboma in neurosurgery. Case report and literature review. Neurocirugia (Astur). 2009; 20:44–48.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intracranial Metastases of Cervical Intramedullary Low-Grade Astrocytoma without Malignant Transformation in Adult
- Intracranial Undifferentiated Sarcoma Arising from a Low-Grade Glioma: A Case Report and Literature Review
- Gossypiboma Mimicking a Soft Tissue Tumor
- Surgical Experience of Multiple Recurrent Astrocytoma: Case Report
- A Case of Astrocytoma in the Corpus Callosum
