J Korean Med Assoc.
2008 Nov;51(11):1051-1060. 10.5124/jkma.2008.51.11.1051.
Advances in Endoscopic Treatment of Children with Vesicoureteral Reflux
- Affiliations
-
- 1Department of Urology, Seoul National University College of Medicine, Korea. hchoi@snu.ac.kr
- 2Department of Urology, Konkuk University College of Medicine, Korea. bminki@yahoo.co.kr
- KMID: 2137748
- DOI: http://doi.org/10.5124/jkma.2008.51.11.1051
Abstract
- Vesicoureteral reflux (VUR) is a common cause of urinary tract infection in children. The primary goals of managing VUR are to prevent pyelonephritis, renal damage, and long-term complications. Management may be either medical or surgical. The rationale of medical therapy is that spontaneous resolution of reflux often occurs with time. Surgical therapy is based on the principle that eliminating the reflux will minimize the likelihood of renal damage and other reflux related complications. Open ureteral reimplantation is 95~98% effective for correcting reflux, and has been the standard surgical treatment for many years. In recent years, the management of VUR has changed dramatically, mostly because of the widespread acceptance of endoscopic treatment. Optimal materials for endoscopic treatment need to be easy to inject, nontoxic, and not to migrate to other organs, result in minimal local inflammation, and be well encapsulated. Since the first clinical application of endoscopic treatment for VUR in 1984 employed subureteric polytetrafluoroethylene injection, the materials and techniques have improved considerably. Following the approval of dextranomer/hyaluronic acid by the U.S. Food and Drug Administration in 2001, the endoscopic treatment of VUR has become increasingly popular in many parts of the world. The combination of increased success, minimal morbidity, a reasonable safety profile, and short operative time has strengthened the role of endoscopic treatment for VUR. The long-term durability and reproducibility of results will make endoscopic treatment an effective alternative to antibiotic prophylaxis in low-grade reflux and to open surgery in high-grade reflux.
Keyword
MeSH Terms
Figure
-
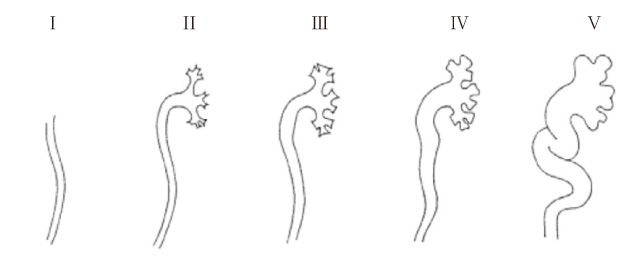
Figure 1 International classification of vesicoureteral reflux (International Reflux Study Committee, 1981).

Figure 2 (A) Percent change of reflux persistence, grades I, II and IV, for 1 to 5 years following presentation (B) Percent change of reflux persistence by age at presentation, grades III, for 1 to 5 years following presentation (The AUA pediatric vesicoureteral reflux clinical guidelines panel, 1997).
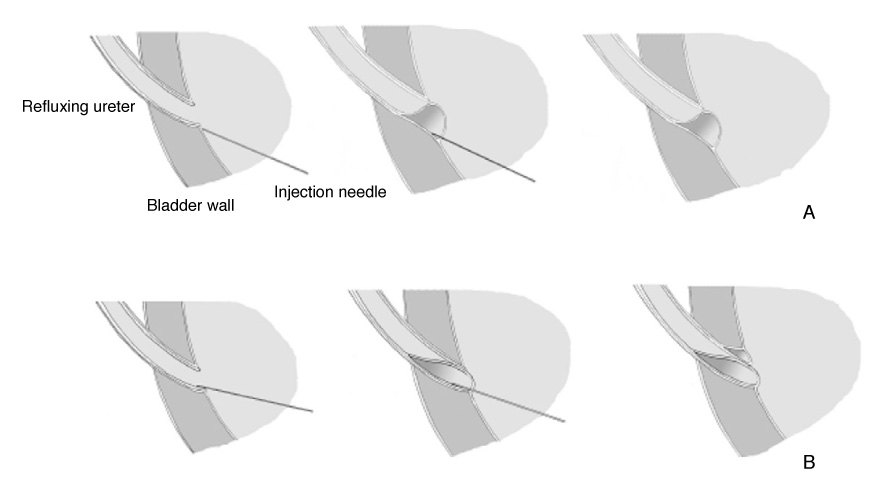
Figure 3 (A) Subureteric injection technique. (B) Hydrodistention-implantation technique.
Reference
-
1. Medical versus surgical treatment of primary vesicoureteral reflux: report of the International Reflux Study Committee. Pediatrics. 1981. 67:392–400.2. Elder JS, Peters CA, Arant BS Jr, Ewalt DH, Hawtrey CE, Hurwitz RS, Parrott TS, Snyder HM 3rd, Weiss RA, Woolf SH, Hasselblad V. Pediatric Vesicoureteral Reflux Guidelines Panel summary report on the management of primary vesicoureteral reflux in children. J Urol. 1997. 157:1846–1851.
Article3. Hensle TW, Hyun G, Grogg AL, Eaddy M. Part 2: Examining pediatric vesicoureteral reflux: a real-world evaluation of treatment patterns and outcomes. Curr Med Res Opin. 2007. 23:Suppl 4. S7–S13.
Article4. Conway PH, Cnaan A, Zaoutis T, Henry BV, Grundmeier RW, Keren R. Recurrent urinary tract infections in children: risk factors and association with prophylactic antimicrobials. JAMA. 2007. 298:179–186.5. O'Donnell B, Puri P. Treatment of vesicoureteric reflux by endoscopic injection of Teflon. Br Med J. 1984. 289:7–9.6. Caldamone AA, Diamond DA. Long-term results of the endoscopic correction of vesicoureteral reflux in children using autologous chondrocytes. J Urol. 2001. 165:2224–2227.
Article7. Aaronson IA, Rames RA, Greene WB, Walsh LG, Hasal UA, Garen PD. Endoscopic treatment of reflux: migration of Teflon to the lungs and brain. Eur Urol. 1993. 23:394–399.
Article8. Haferkamp A, Contractor H, Mohring K, Staehler G, Dorsam J. Failure of subureteral bovine collagen injection for the endoscopic treatment of primary vesicoureteral reflux in long-term follow-up. Urology. 2000. 55:759–763.
Article9. Henly DR, Barrett DM, Weiland TL, O'Connor MK, Malizia AA, Wein AJ. Particulate silicone for use in periurethral injections: local tissue effects and search for migration. J Urol. 1995. 153:2039–2043.
Article10. Tarcan T, Tinay I, Temiz Y, Simsek F. Long-term results of endoscopic treatment of vesicoureteral reflux with the subureteric injection of calcium hydroxyapatite. Int Urol Nephrol. 2007. 39:1011–1014.
Article11. Stenberg A, Lackgren G. A new bioimplant for the endoscopic treatment of vesicoureteral reflux: experimental and short-term clinical results. J Urol. 1995. 154:800–803.
Article12. Lackgren G, Wahlin N, Skoldenberg E, Stenberg A. Long-term followup of children treated with dextranomer/hyaluronic acid copolymer for vesicoureteral reflux. J Urol. 2001. 166:1887–1892.
Article13. Kirsch AJ, Perez-Brayfield M, Smith EA, Scherz HC. The modified sting procedure to correct vesicoureteral reflux: improved results with submucosal implantation within the intramural ureter. J Urol. 2004. 171:2413–2416.
Article14. Puri P, Pirker M, Mohanan N, Dawrant M, Dass L, Colhoun E. Subureteral dextranomer/hyaluronic acid injection as first line treatment in the management of high grade vesicoureteral reflux. J Urol. 2006. 176:1856–1859.
Article15. Elder JS, Diaz M, Caldamone AA, Cendron M, Greenfield S, Hurwitz R, Kirsch A, Koyle MA, Pope J, Shapiro E. Endoscopic therapy for vesicoureteral reflux: a meta-analysis. I. Reflux resolution and urinary tract infection. J Urol. 2006. 175:716–722.
Article16. Stenberg A, Lackgren G. Treatment of vesicoureteral reflux in children using stabilized non-animal hyaluronic acid/dextranomer gel (NASHA/DX): A long-term observational study. J Pediatr Urol. 2007. 3:80–85.
Article17. Lendvay TS, Sorensen M, Cowan CA, Joyner BD, Mitchell MM, Grady RW. The evolution of vesicoureteral reflux management in the era of dextranomer/hyaluronic acid copolymer: a pediatric health information system database study. J Urol. 2006. 176:1864–1867.
Article
