A Gastric Composite Tumor with an Adenocarcinoma and a Neuroendocrine Carcinoma: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, Bong Seng Memorial Hospital, Busan, Korea.
- 2Department of Internal Medicine, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea. luckyace@hanmail.net
- KMID: 2048934
- DOI: http://doi.org/10.5946/ce.2013.46.3.280
Abstract
- A 70-year-old woman was admitted to our department with epigastric discomfort and nausea over the duration of 1 month. An esophagogastroduodenoscopy showed the presence of a 1.0x1.0 cm-sized flat lesion with central ulceration at the greater curvature side of the antrum. A biopsy demonstrated the presence of an adenocarcinoma of well differentiated, intestinal type in the stomach. Endoscopic submucosal dissection was done and the diagnosis of a composite neuroendocrine carcinoma with an adenocarcinoma of the stomach was confirmed. We report a case of a gastric composite tumor with an adenocarcinoma and neuroendocrine carcinoma confirmed by endoscopic submucosal dissection with a review of the literature.
MeSH Terms
Figure
-
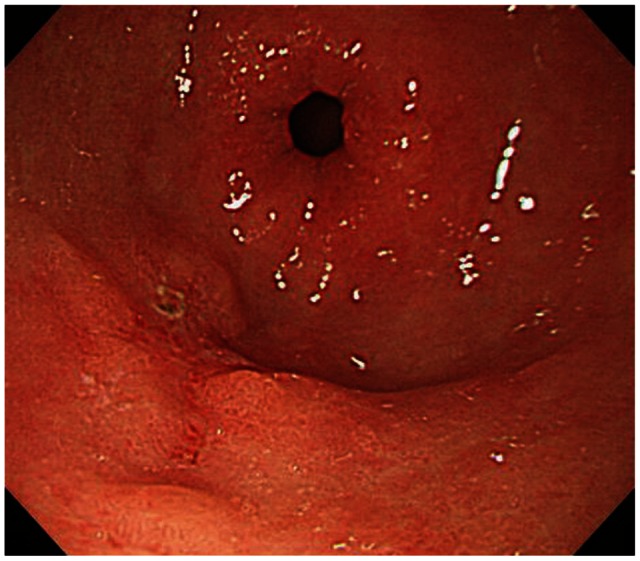
Fig. 1 The esophagogastroduodenoscopy finding. The picture showed a 1.0×1.0-cm-sized ulcerative mucosal lesion at the greater curvature side of the distal antrum.
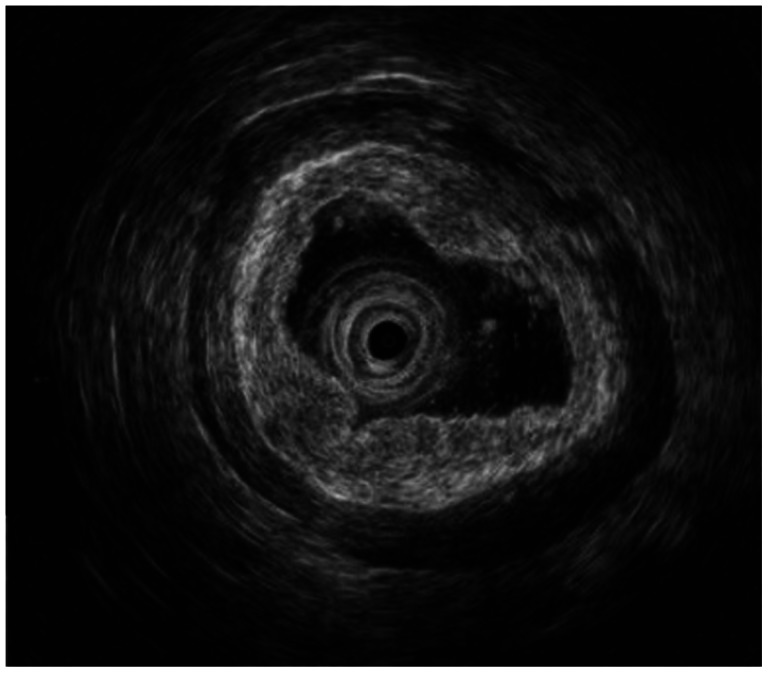
Fig. 2 The patient underwent endoscopic ultrasound. The picture revealed a 1-cm-sized isoechoic mass in the mucosal layer of the greater curvature of the distal antrum.
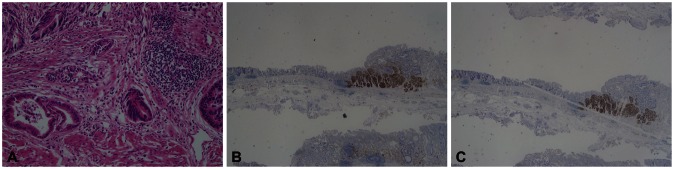
Fig. 3 Pathologic findings. (A) It shows a well-differentiated adenocarcinoma and a neuroendocrine carcinoma. One area of transition between the two histologic types was observed (H&E stain, ×200). (B) The tumor cells with endocrine differentiation are highlighted by CD 56 stain, but adenocarcinoma shows no immunoreactivity (CD 56 stain, ×40). (C) The tumor cells with endocrine differentiation are highlighted by synaptophysin stain, but adenocarcinoma shows no immunoreactivity (synaptophysin stain, ×40).
Cited by 1 articles
-
Mixed adenoneuroendocrine carcinoma in the stomach: a case report with a literature review
Ki Hyun Kim, Hyun Jung Lee, Si Hak Lee, Sun-Hwi Hwang
Ann Surg Treat Res. 2018;94(5):270-273. doi: 10.4174/astr.2018.94.5.270.
Reference
-
1. Reis-Filho JS, Schmitt FC. Amphicrine gastric carcinoma. Arch Pathol Lab Med. 2001; 125:1513–1514. PMID: 11698020.
Article2. Yamashina M, Flinner RA. Concurrent occurrence of adenocarcinoma and carcinoid tumor in the stomach: a composite tumor or collision tumors? Am J Clin Pathol. 1985; 83:233–236. PMID: 3969962.
Article3. Lewin K. Carcinoid tumors and the mixed (composite) glandular-endocrine cell carcinomas. Am J Surg Pathol. 1987; 11(Suppl 1):71–86. PMID: 3544888.
Article4. Strofilas A, Dalianoudis IG, Lagoudianakis EE, et al. Collision tumour of the stomach with a cancer to cancer metastasis: a case report. Cases J. 2008; 1:63. PMID: 18662400.
Article5. Morishita Y, Sugitani M, Sheikh A, Nemoto N, Fujii M, Takayama T. Collision tumor of the stomach: a rare case of an adenocarcinoma and carcinoid tumor. Arch Pathol Lab Med. 2005; 129:407–409. PMID: 15737041.
Article6. Kim EY, Park KC, Kwon JG. A case of double primary cancer: early gastric adenocarcinoma associated with adenocarcinoma and carcinoid. Korean J Gastroenterol. 2003; 42:533–538. PMID: 14695711.7. Liu SW, Chen GH, Hsieh PP. Collision tumor of the stomach: a case report of mixed gastrointestinal stromal tumor and adenocarcinoma. J Clin Gastroenterol. 2002; 35:332–334. PMID: 12352297.8. Fukui H, Takada M, Chiba T, et al. Concurrent occurrence of gastric adenocarcinoma and duodenal neuroendocrine cell carcinoma: a composite tumour or collision tumours? Gut. 2001; 48:853–856. PMID: 11358908.9. Levendoglu H, Cox CA, Nadimpalli V. Composite (adenocarcinoid) tumors of the gastrointestinal tract. Dig Dis Sci. 1990; 35:519–525. PMID: 2180655.
Article10. Fujiyoshi Y, Kuhara H, Eimoto T. Composite glandular-endocrine cell carcinoma of the stomach. Report of two cases with goblet cell carcinoid component. Pathol Res Pract. 2005; 200:823–829. PMID: 15792127.
Article11. Granberg D, Wilander E, Stridsberg M, Granerus G, Skogseid B, Oberg K. Clinical symptoms, hormone profiles, treatment, and prognosis in patients with gastric carcinoids. Gut. 1998; 43:223–228. PMID: 10189848.
Article12. Volante M, Rindi G, Papotti M. The grey zone between pure (neuro)endocrine and non-(neuro)endocrine tumours: a comment on concepts and classification of mixed exocrine-endocrine neoplasms. Virchows Arch. 2006; 449:499–506. PMID: 17033797.
Article13. Klöppel G, Perren A, Heitz PU. The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification. Ann N Y Acad Sci. 2004; 1014:13–27. PMID: 15153416.14. Rindi G, Luinetti O, Cornaggia M, Capella C, Solcia E. Three subtypes of gastric argyrophil carcinoid and the gastric neuroendocrine carcinoma: a clinicopathologic study. Gastroenterology. 1993; 104:994–1006. PMID: 7681798.
Article15. Gilligan CJ, Lawton GP, Tang LH, West AB, Modlin IM. Gastric carcinoid tumors: the biology and therapy of an enigmatic and controversial lesion. Am J Gastroenterol. 1995; 90:338–352. PMID: 7872269.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Composite Neuroendocrine Carcinoma with Adenocarcinoma of the Stomach Misdiagnosed as a Giant Submucosal Tumor
- A Case of a Gastric Composite Tumor with an Adenocarcinoma and a Large Cell Neuroendocrine Carcinoma
- Gastric Collision Tumor (Adenocarcinoma and Neuro-endocrine Carcinoma): A Report of Two Cases
- Gastric Adenocarcinoma with Coexistent Hepatoid Adenocarcinoma and Neuroendocrine Carcinoma: A Case Report
- Gastric Collision Tumor Consisting of Mucinous Carcinoma and Large Cell Neuroendocrine Carcinoma: A Case Report
