Gastric Collision Tumor Consisting of Mucinous Carcinoma and Large Cell Neuroendocrine Carcinoma: A Case Report
- Affiliations
-
- 1Department of Radiology, Bundang Jesaeng General Hospital, Korea. leechoii@paran.com
- 2Department of Pathology, Bundang Jesaeng General Hospital, Korea.
- KMID: 2097899
- DOI: http://doi.org/10.3348/jksr.2010.63.3.239
Abstract
- The concurrence of two different pathological tumors of the stomach is infrequent. Even rarer is a gastric collision tumor of both tumor types. Although there have been a few reported cases of gastric collision tumors that consisted of an adenocarcinoma and neuroendocrine carcinoma, to the best of our knowledge, there is no documented case report of a gastric collision tumor consisting of a mucinous carcinoma and large cell neuroendocrine carcinoma. We report a case of gastric collision tumor, consisting of a mucinous carcinoma and large cell neuroendocrine carcinoma that presented as abdominal discomfort in a 64-year-old man. This finding draws attention to the related findings from previous studies on gastric collision tumors.
MeSH Terms
Figure
-
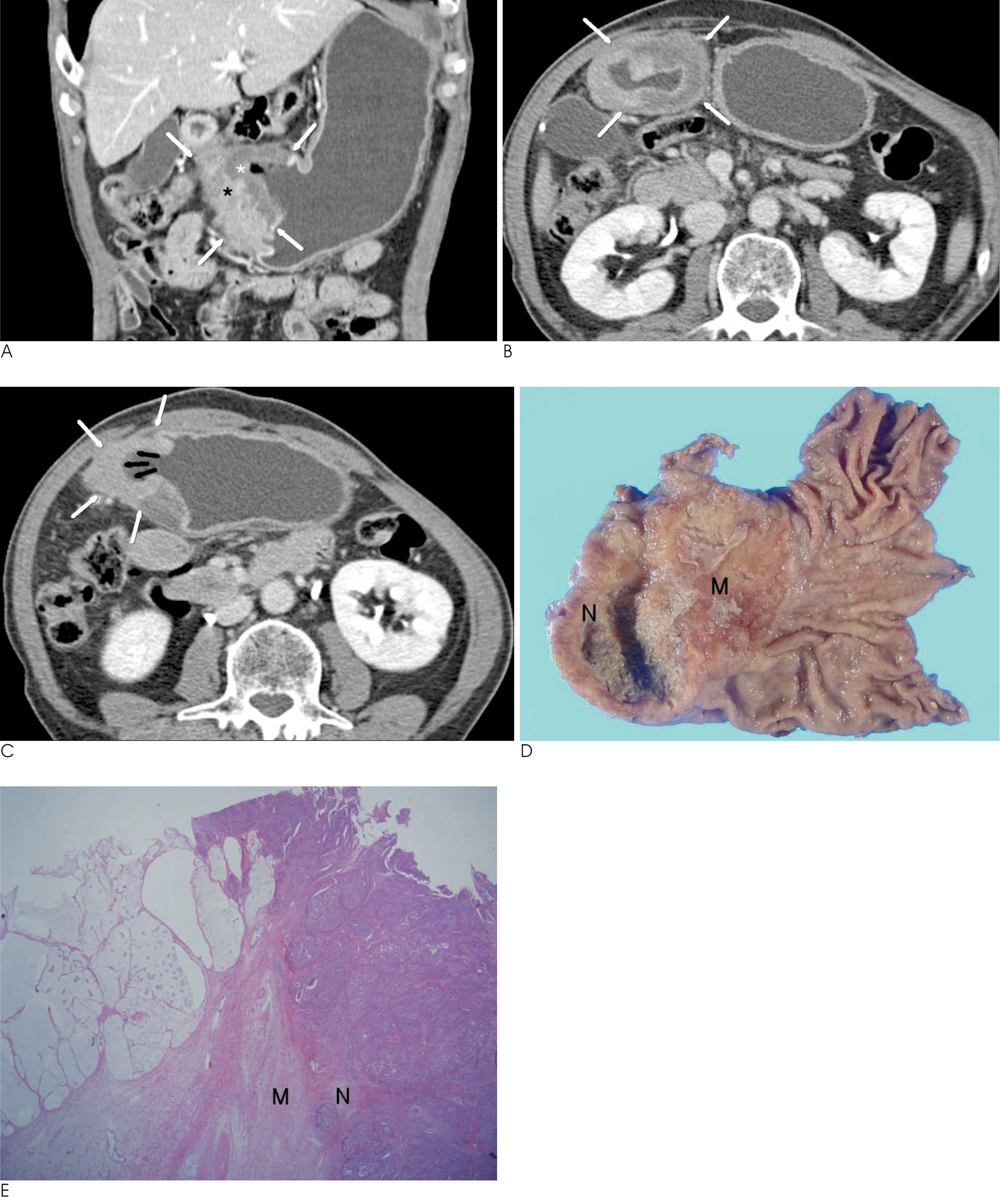
Fig. 1 A 64-year-old man with a mucinous carcinoma and neuroendocrine carcinoma of the stomach. A. Contrast-enhanced coronal CT scan obtained during the portal venous phase shows focal wall thickening (white arrows) at the antrum. Note the border between the mucinous carcinoma (white asterisk) and neuroendocrine carcinoma (black asterisk). B. Contrast-enhanced axial CT scan obtained during the delayed phase shows focal wall thickening (white arrows) at anterior and posterior wall of the proximal antrum, particularly in the low-attenuating middle or outer layer, with more than 50% preservation of the thin high-attenuating inner layer. The layered enhancement pattern is shown. C. Contrast-enhanced axial CT scan obtained during the delayed phase shows well-enhancing, focal wall thickening (white arrows) with depression (black arrows) at anterior and posterior wall of the distal antrum. The homogeneous enhancement pattern is shown. D. Gross photography shows a large ulceroinfiltrative mass (Borrmann type 3) in antrum. Two distinct lesions were identified. One is the gelatinous and glistening mass (M) at lesser curvature, anterior and posterior wall of the proximal antrum, and the other is the firm mass (N) at greater curvature, anterior and posterior wall of the distal antrum. E. Microscopically, the tumors are composed of two distinct neoplastic cell component. Mucinous carcinoma shows the mucinous lakes containing floating cell clusters, and neuroendocrine carcinoma shows the tumor nest with central necrosis (data not shown). There is a no admixture at the border between the neuroendocrine carcinoma (N) and mucinous carcinoma (M) (H & E; ×12.5).
Reference
-
1. Park MS, Yu JS, Kim MJ, Noh TW, Lee KH, Lee JT, et al. Mucinous versus nonmucinous gastric carcinoma: differentiation with helical CT. Radiology. 2002; 223:540–546.2. Park BS, Jo TY, Seo HI, Kim HS, Kim DH, Jeon TY, Kim DH, Sim MS, Kim JY. Gastric Collision Tumor (Adenocarcinoma and Neuroendocrine carcinoma) Diagnosed as a Advanced Gastric Cancer. J Korean Surg Soc. 2007; 73:173–177.3. Kwak HS, Lee JM, Lee YH, Kim YK, Kim CS. Gastric neuroendocrine carcinoma presenting as a wandering exophytic mass: a case report. J Korean Radiol Soc. 2002; 47:217–220.4. Kim HS, Hong SS, Kim JH, Jin SY, Choi DL, Kim YJ, Kwon KH. CT Gastrography Findings of a Gastric Collision Tumor that Consisted of an Adenocarcinoma and Neuroendocrine Tumor: A Case Report. J Korean Radiol Soc. 2007; 57:463–466.5. Kim EY, Park KC, Kwon JG. A case of double primary cancer: early gastric adenocarcinoma associated with adenocarcinoma and carcinoid. Korean J Gastroenterol. 2003; 42:533–538.6. Hirano Y, Hara T, Nozawa H, Oyama K, Ohta N, Omura K, et al. Combined choriocarcinoma, neuroendocrine cell carcinoma and tubular adenocarcinoma in the stomach. World J Gastroenterol. 2008; 14:3269–3272.7. Liu SW, Chen GH, Hsieh PP. Collision tumor of the stomach: a case report of mixed gastrointestinal stromal tumor and adenocarcinoma. J Clin Gastroenterol. 2002; 35:332–334.8. Kim HJ, Choi DG, Lee SJ, Lee WJ, Kim S, Kim JJ, et al. Four cases of large cell neuroendocrine carcinoma of the stomach: findings on CT and barium studies. A case report. J Korean Radiol Soc. 2008; 58:607–612.9. Choi JS, Kim MA, Lee HE, Lee HS, Kim WH. Mucinous gastric carcinomas: clinicopathologic and molecular analyses. Cancer. 2009; 115:3581–3590.10. Jung JH, Kim AY, Kim HJ, Yook JH, Yu ES, Jang YJ, Park SH, Shin YM, Ha HK. Multidetector CT of Locally Invasive Advanced Gastric Cancer: Value of Oblique Coronal Reconstructed Images for the Assessment of Local Invasion. J Korean Soc Radiol. 2010; 62:47–55.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ovarian Large Cell Neuroendocrine Carcinoma Associated with Endocervical-like Mucinous Borderline Tumor: A Case Report and Literature Review
- Pancreatic Collision Tumor of Desmoid-Type Fibromatosis and Mucinous Cystic Neoplasm: A Case Report
- A Case of a Collision Tumor in the Ampulla of Vater with an Adenocarcinoma and a Large Cell Neuroendocrine Carcinoma
- Gastric Collision Tumor (Adenocarcinoma and Neuro-endocrine Carcinoma): A Report of Two Cases
- Large cell Neuroendocrine Carcinoma Associated with Invasive Mucinous Adenocarcinoma of the Uterine Cervix
