Anti-VEGF-refractory Exudative Age-related Macular Degeneration: Differential Response According to Features on Optical Coherence Tomography
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. sejoon1@hanmail.net
- KMID: 1792078
- DOI: http://doi.org/10.3341/kjo.2013.27.6.425
Abstract
- PURPOSE
To describe optical coherence tomography (OCT) characteristics of neovascular age-related macular degeneration (AMD) patients refractory to intravitreal anti-vascular endothelial growth factor (VEGF) injections (ranibizumab, bevacizumab) and their responses to alternative anti-VEGF agents or photodynamic therapy (PDT).
METHODS
A retrospective review of 267 neovascular AMD patients treated with intravitreal anti-VEGF injections.
RESULTS
Twenty patients (7.5%) were refractory to anti-VEGF injections (stationary or increased retinal exudation despite three or more monthly injections). They were grouped into either the extensive intraretinal fluid group (IRF group, 9 patients) or the subretinal fluid only group (SRF group, 11 patients) according to OCT findings. In the IRF group, response rates to subsequent treatment were 0% (0 / 7) for bevacizumab, 50% (3 / 6) for ranibizumab and 50% (3 / 6) for PDT +/- anti-VEGF. Three out of four bevacizumab-refractory patients showed response to ranibizumab as a secondary treatment. In the SRF group, response rates were lower with 0% (0 / 7) for bevacizumab, 22.2% (2 / 9) for ranibizumab and 28.6% (2 / 7) for PDT +/- anti-VEGF. One out of four bevacizumab-refractory patients responded to ranibizumab. The visual outcome was worse in the IRF group (median 20 / 1,000) than in the SRF group (median 20 / 100).
CONCLUSIONS
In anti-VEGF-refractory neovascular AMD, patients with extensive IRF refractory to bevacizumab can be responsive to ranibizumab while patients with SRF may be refractory to both, suggesting a different pathophysiology and intraocular pharmacokinetics.
Keyword
MeSH Terms
-
Aged
Aged, 80 and over
Angiogenesis Inhibitors/administration & dosage
Antibodies, Monoclonal, Humanized/*administration & dosage
Female
Fluorescein Angiography
Follow-Up Studies
Fundus Oculi
Humans
Intravitreal Injections
Male
Middle Aged
Retrospective Studies
Tomography, Optical Coherence/*methods
Treatment Outcome
Vascular Endothelial Growth Factor A/*antagonists & inhibitors
Visual Acuity
Wet Macular Degeneration/*drug therapy/metabolism/pathology
Angiogenesis Inhibitors
Antibodies, Monoclonal, Humanized
Vascular Endothelial Growth Factor A
Figure
-

Fig. 1 Case 7. A 65-year-old male diagnosed with polypoidal choroidal vasculopathy (A, fundus photography; B, fluorescein angiography). His initial visual acuity was 20 / 500, and findings compatible with polypoidal choroidal vasculopathy were observed on indocyanine green angiography (C). Optical coherence tomography (D) showed extensive intraretinal fluid. He was refractory to six sequential bevacizumab injections and was treated with combined photodynamic therapy and bevacizumab injections twice without success (E, optical coherence tomography). The patient received ranibizumab injections monthly, effectively decreasing the intraretinal fluid (F, optical coherence tomography), although his visual acuity was limited to 20 / 1,000.

Fig. 2 Case 11. A 76-year-old male diagnosed with occult choroidal neovascularization (A, fundus photography; B, fluorescein angiography). His visual acuity was 20 / 50, and he showed no evidence of polypoidal choroidal vasculopathy on indocyanine green angiography (C). Optical coherence tomography (D) revealed subretinal fluid only. The patient was refractory to three sequential ranibizumab injections and received combined photodynamic therapy and ranibizumab injections, which also had no effect (E, optical coherence tomography). He was prescribed additional ranibizumab injections, but the SRF still remained (F, optical coherence tomography). At the last follow-up visit, his visual acuity was 20 / 100.
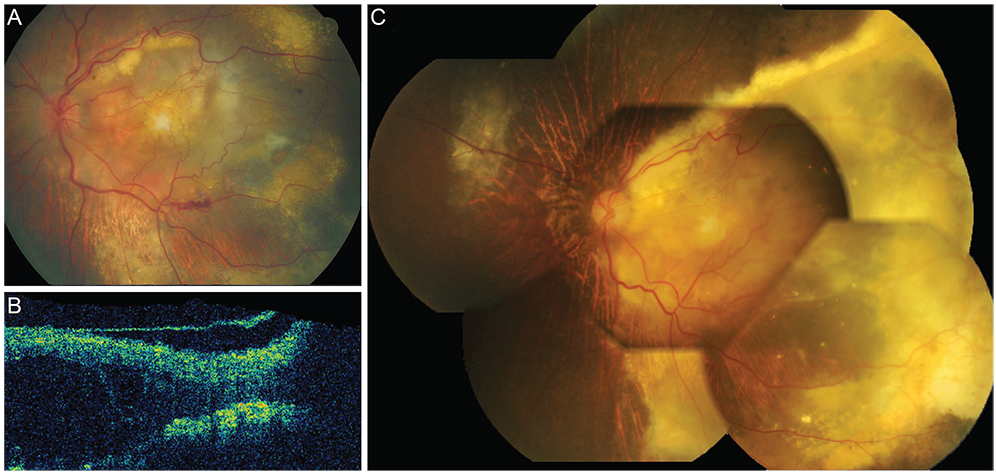
Fig. 3 A 78-year-old female diagnosed with occult choroidal neovascularization with extensive exudation (A, fundus photography; B, optical coherence tomography). In six years, the exudation progressed to involve a larger area, encompassing more than half of the retina (C, fundus photography).
Reference
-
1. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006; 355:1419–1431.2. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006; 355:1432–1444.3. Abraham-Marin ML, Cortes-Luna CF, Alvarez-Rivera G, et al. Intravitreal bevacizumab therapy for neovascular age-related macular degeneration: a pilot study. Graefes Arch Clin Exp Ophthalmol. 2007; 245:651–655.4. Avery RL, Pieramici DJ, Rabena MD, et al. Intravitreal bevacizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmology. 2006; 113:363–372.e5.5. Costa RA, Jorge R, Calucci D, et al. Intravitreal bevacizumab for choroidal neovascularization caused by AMD (IBeNA Study): results of a phase 1 dose-escalation study. Invest Ophthalmol Vis Sci. 2006; 47:4569–4578.6. Fong DS, Custis P, Howes J, Hsu JW. Intravitreal bevacizumab and ranibizumab for age-related macular degeneration a multicenter, retrospective study. Ophthalmology. 2010; 117:298–302.7. Rich RM, Rosenfeld PJ, Puliafito CA, et al. Short-term safety and efficacy of intravitreal bevacizumab (Avastin) for neovascular age-related macular degeneration. Retina. 2006; 26:495–511.8. Fung AE, Lalwani GA, Rosenfeld PJ, et al. An optical coherence tomography-guided, variable dosing regimen with intravitreal ranibizumab (Lucentis) for neovascular age-related macular degeneration. Am J Ophthalmol. 2007; 143:566–583.9. Brown DM, Regillo CD. Anti-VEGF agents in the treatment of neovascular age-related macular degeneration: applying clinical trial results to the treatment of everyday patients. Am J Ophthalmol. 2007; 144:627–637.10. Cho M, Barbazetto IA, Freund KB. Refractory neovascular age-related macular degeneration secondary to polypoidal choroidal vasculopathy. Am J Ophthalmol. 2009; 148:70–78.e1.11. Mojana F, Cheng L, Bartsch DU, et al. The role of abnormal vitreomacular adhesion in age-related macular degeneration: spectral optical coherence tomography and surgical results. Am J Ophthalmol. 2008; 146:218–227.12. Treatment of age-related macular degeneration with photodynamic therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: one-year results of 2 randomized clinical trials--TAP report. Arch Ophthalmol. 1999; 117:1329–1345.13. Lux A, Llacer H, Heussen FM, Joussen AM. Non-responders to bevacizumab (Avastin) therapy of choroidal neovascular lesions. Br J Ophthalmol. 2007; 91:1318–1322.14. CATT Research Group. Martin DF, Maguire MG, et al. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011; 364:1897–1908.15. Stangos AN, Gandhi JS, Nair-Sahni J, et al. Polypoidal choroidal vasculopathy masquerading as neovascular age-related macular degeneration refractory to ranibizumab. Am J Ophthalmol. 2010; 150:666–673.16. Gaudreault J, Fei D, Beyer JC, et al. Pharmacokinetics and retinal distribution of ranibizumab, a humanized antibody fragment directed against VEGF-A, following intravitreal administration in rabbits. Retina. 2007; 27:1260–1266.17. Kofoed-Enevoldsen A, Foyle WJ, Fernandez M, Yudkin JS. Evidence of impaired glomerular charge selectivity in nondiabetic subjects with microalbuminuria: relevance to cardiovascular disease. Arterioscler Thromb Vasc Biol. 1996; 16:450–454.18. Nishihara H. Studies on the ultrastructure of the inner limiting membrane of the retina: distribution of anionic sites in the inner limiting membrane of the retina. Nihon Ganka Gakkai Zasshi. 1991; 95:951–958.19. Bunt-Milam AH, Saari JC, Klock IB, Garwin GG. Zonulae adherentes pore size in the external limiting membrane of the rabbit retina. Invest Ophthalmol Vis Sci. 1985; 26:1377–1380.20. Kim H, Robinson SB, Csaky KG. FcRn receptor-mediated pharmacokinetics of therapeutic IgG in the eye. Mol Vis. 2009; 15:2803–2812.21. Heiduschka P, Fietz H, Hofmeister S, et al. Penetration of bevacizumab through the retina after intravitreal injection in the monkey. Invest Ophthalmol Vis Sci. 2007; 48:2814–2823.22. Shahar J, Avery RL, Heilweil G, et al. Electrophysiologic and retinal penetration studies following intravitreal injection of bevacizumab (Avastin). Retina. 2006; 26:262–269.23. Brasil OF, Smith SD, Galor A, et al. Predictive factors for short-term visual outcome after intravitreal triamcinolone acetonide injection for diabetic macular oedema: an optical coherence tomography study. Br J Ophthalmol. 2007; 91:761–765.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Optical Coherence Tomography Characteristics among Three Subtypes of Exudative Age-related Macular Degeneration
- Optical Coherence Tomography of Idiopathic Polypoidal Choroidal Vasculopathy
- High Dose Intravitreal Bevacizumab for Refractory Pigment Epithelial Detachment in Age-related Macular Degeneration
- Anatomical Characteristics of End-stage Exudative Age-related Macular Degeneration Refractory to Intravitreal Anti-vascular Endothelial Growth Factor Injection
- Longitudinal Changes in Retinal Nerve Fiber Layer Thickness after Intravitreal Anti-vascular Endothelial Growth Factor Therapy
