Radiologic Findings of Immunoglobulin G4 Related Sclerosing Esophagitis: A Case Report
- Affiliations
-
- 1Department of Radiology, Inje University Ilsanpaik Hospital, Inje University College of Medicine, Goyang, Korea. sykim@paik.ac.kr
- KMID: 1439406
- DOI: http://doi.org/10.3348/jksr.2012.66.2.149
Abstract
- We describe a case of immunoglobulin G4 (IgG4)-related sclerosing esophagitis occurring in a 63-year-old man with progressive dysphagia and 10-kg weight loss over 9 months. An esophagoscopy revealed significant stricture with diffuse mucosal friability and ulceration at mid esophagus level. Barium esophagogram showed diffuse stenosis at the mid and lower esophagus levels with ulcerations and irregularity of the mucosa. Multidetector computed tomography revealed diffuse edematous and circumferential thickening of the submucosa and muscle layer of this esophageal segment. Fluorine 18 fluorodeoxyglucose positron emission tomography (FDG PET) revealed diffuse mild FDG uptake in mid to lower esophagus. Although benign inflammatory lesion was suspected based on the imaging findings, the patient underwent surgery for worsening esophageal stricture and the esophageal lesion was pathologically confirmed as IgG4-related sclerosing esophagitis. Radiologic benignancy and high clinical suspicion for IgG4-related sclerosing disease may help making a proper decision and avoiding unnecessary operation.
MeSH Terms
-
Barium
Constriction, Pathologic
Deglutition Disorders
Esophageal Stenosis
Esophagitis
Esophagoscopy
Esophagus
Fluorodeoxyglucose F18
Humans
Immunoglobulin G
Immunoglobulins
Middle Aged
Mucous Membrane
Multidetector Computed Tomography
Muscles
Positron-Emission Tomography
Ulcer
Weight Loss
Barium
Fluorodeoxyglucose F18
Immunoglobulin G
Immunoglobulins
Figure
-

Fig. 1 Right lateral oblique image of an esophagography shows smooth stricture at the and lower esophageal level with mucosal irregularity. Ulceration is noted at the stenotic portion of the mid esophagus level (arrowhead).
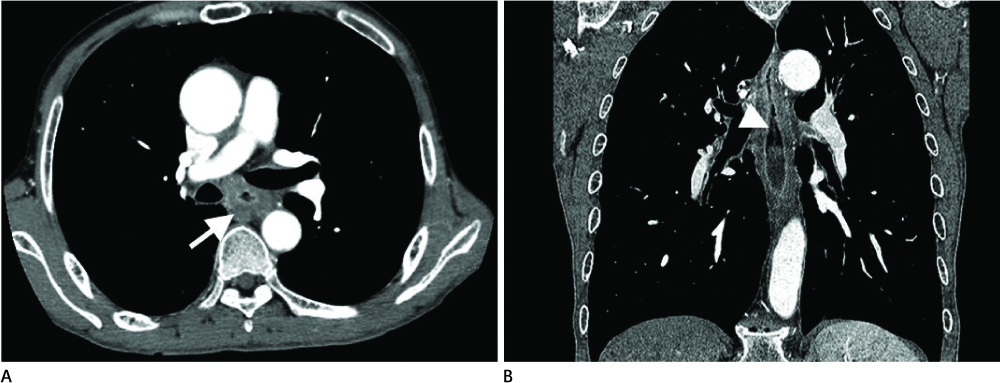
Fig. 2 A 63-year-old man with progressive dysphagia and 10 kg weight loss for 9 months. (A) Axial and (B) reformatted coronal images of a 64 slice MDCT with enhancement demonstrate circumferential edematous thickening in the submucosa and muscle layer (arrow) with mucosal enhancement (arrowhead) involving a long segment of the mid and distal esophagus. Note.-MDCT = multidetector computed tomography
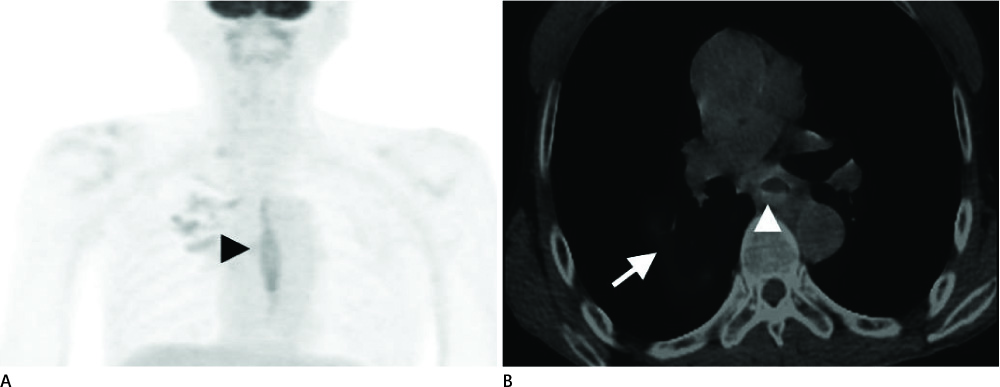
Fig. 3 PET images. A. MIP image of 18F-FDG PET shows diffuse mild FDG uptake at the mid and distal esophagus level (arrowhead). B. PET/CT fusion image shows mild FDG uptake in the esophageal mucosa at the subcarinal level (arrowhead). Mild FDG uptake is also demonstrated in active tuberculosis lesions of the right lung (arrow). Note.-18F-FDG PET = 18F-fluorodeoxyglucose positron emission tomography, MIP = Maximum-Intensity-Projection

Fig. 4 Microscopically, the stenotic esophageal segment shows transmural fibrosing inflammation with extensive mucosal ulceration and lymphoid follicles (H&E, × 40). There are abundant IgG4-positive plasma cells (inset, × 400, IgG4 immunostaining). Note.-IgG4 = immunoglobulin G4
Reference
-
1. Kamisawa T, Okamoto A. IgG4-related sclerosing disease. World J Gastroenterol. 2008; 14:3948–3955.2. Lopes J, Hochwald SN, Lancia N, Dixon LR, Ben-David K. Autoimmune esophagitis: IgG4-related tumors of the esophagus. J Gastrointest Surg. 2010; 14:1031–1034.3. Lee H, Joo M, Song TJ, Chang SH, Kim H, Kim YS, et al. IgG4-related sclerosing esophagitis: a case report. Gastrointest Endosc. 2011; 73:834–837.4. Fujita T, Ando T, Sakakibara M, Hosoda W, Goto H. Refractory gastric ulcer with abundant IgG4-positive plasma cell infiltration: a case report. World J Gastroenterol. 2010; 16:2183–2186.5. Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001; 344:732–738.6. Chen CC. Autoimmune pancreatitis and IgG4-related sclerosing disease: an emerging disease entity. J Chin Med Assoc. 2008; 71:1–3.7. Okazaki K, Uchida K, Matsushita M, Takaoka M. How to diagnose autoimmune pancreatitis by the revised Japanese clinical criteria. J Gastroenterol. 2007; 42:Suppl 18. 32–38.8. Hirano K, Komatsu Y, Yamamoto N, Nakai Y, Sasahira N, Toda N, et al. Pancreatic mass lesions associated with raised concentration of IgG4. Am J Gastroenterol. 2004; 99:2038–2040.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Immunoglobulin G4-Related Sclerosing Disease Mimicking Lung Cancer
- Immunoglobulin G4-related sclerosing cholangitis
- Immunoglobulin G4-Related Systemic Sclerosing Disease: A Case Involving the Ureter and Kidney
- Two Cases of Immunoglobulin G4-Related Sclerosing Disease Mimicking Nasopharyngeal Carcinoma
- Immunoglobulin G4-Related Sclerosing Disease Involving the Urethra: Case Report
