Immunoglobulin G4-Related Sclerosing Disease Involving the Urethra: Case Report
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, and Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul 110-744, Korea. iwishluv@empas.com
- 2Department of Pathology, Seoul National University College of Medicine, Seoul 110-744, Korea.
- KMID: 1397512
- DOI: http://doi.org/10.3348/kjr.2012.13.6.803
Abstract
- Immunoglobulin G4 (IgG4)-related sclerosing disease is a systemic disease characterized by extensive IgG4-positive plasma cells and T-lymphocyte infiltration in various organs. We described the imaging findings of an IgG4-related inflammatory pseudotumor in the urethra. The urethral mass showed isoattenuation on unenhanced CT images, delayed enhancement on enhanced CT images, iso- to slight hyper-intensity on T1 and T2 weighted magnetic resonance images, diffusion restriction on diffusion weighted images, and heterogeneously low echogeneity on ultrasonography.
MeSH Terms
Figure
-
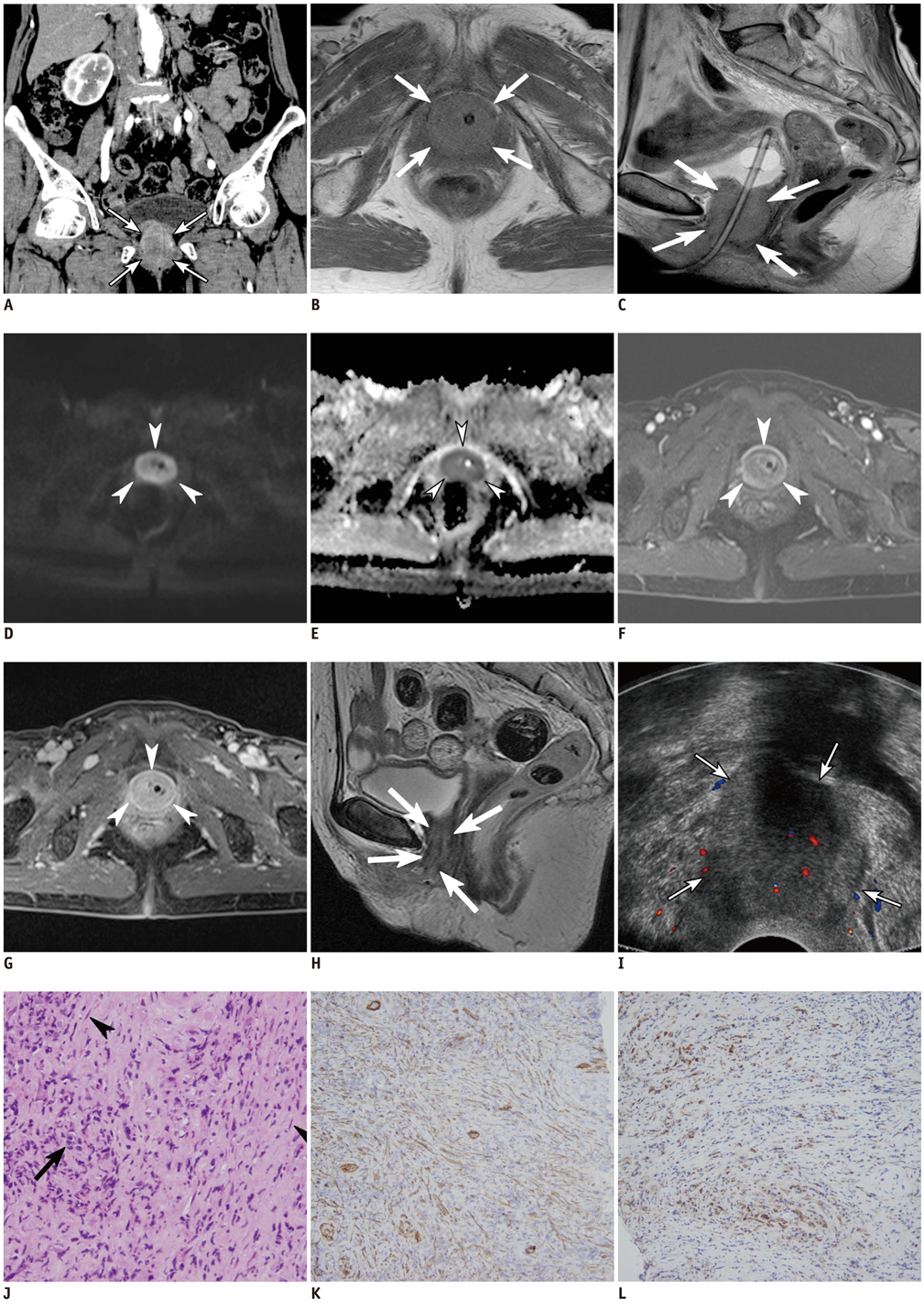
Fig. 1 CT, MR, US, and histologic findings in 72-year-old woman with IgG4-related inflammatory pseudotumor in urethra. A. Coronal reformatted CT image reveals a rim-enhancing soft tissue around urethra (arrows). B. Axial T1-weighted MR image (TR/TE, 790/14) reveals isointense soft tissue (arrows) around urethra. C. Sagittal T2-weighted MR image (TR/TE, 4800/95) reveals iso- to slightly hyperintense mass (arrows) around urethra. D. Axial diffusion weighted MR image (TR/TE, 4800/79) demonstrates intense high signal intensity in urethral mass (arrowheads). E. Axial apparent diffusion coefficient (ADC) map demonstrates concordant low ADC values of urethral mass (arrowheads). F. On gdolinium-enhanced fat-saturation T1-weighted MR images (TR/TE, 2.9/1.2), mass (arrowheads) shows rim-enhncement in arterial phase. G. On 5-minute delayed fat-saturation T1-weighted MR image, mass (arrowheads) shows diffuse enhancement. Note that central portion of mass is enhanced in delayed phase, in comparison with arterial phase image. H. After steroid therapy for three months, sagittal T2-weighted MR image (TR/TE, 4550/107) reveals marked interval decrease in size of urethral mass (arrows). I. Transvaginal ultrasonography image in 72-year-old woman with IgG4-related inflammatory pseudotumor in urethra. transvaginal ultrasonography scan in color Doppler mode reveals heterogeneously low echoic mass (arrows) encasing urethra. Note that vascularity in urethral mass is poor. J. Microscopic exam shows linear spindle cell (arrowheads) proliferation and lymphocyte (arrow) infiltration (Hematoxylin & Eosin, × 200). K. Immunohistochemical staining reveals positivity (brown color) for marker of proliferated spindle cells and smooth muscle actin, suggesting that specimen is compatible with IPT. L. Immunohistochemical staining for IgG4 demonstrates positivity (brown color) in some inflammatory cells and spindle cells, suggesting that specimen is associated with IgG4-related sclerosing disease. IgG4 = immunoglobulin G4, IPT = inflammatory pseudotumor.
Reference
-
1. Kamisawa T, Okamoto A. IgG4-related sclerosing disease. World J Gastroenterol. 2008. 14:3948–3955.2. Kamisawa T, Nakajima H, Egawa N, Funata N, Tsuruta K, Okamoto A. IgG4-related sclerosing disease incorporating sclerosing pancreatitis, cholangitis, sialadenitis and retroperitoneal fibrosis with lymphadenopathy. Pancreatology. 2006. 6:132–137.3. Leporati P, Landek-Salgado MA, Lupi I, Chiovato L, Caturegli P. IgG4-related hypophysitis: a new addition to the hypophysitis spectrum. J Clin Endocrinol Metab. 2011. 96:1971–1980.4. Higashiyama T, Nishida Y, Ugi S, Ishida M, Nishio Y, Ohji M. A case of extraocular muscle swelling due to IgG4-related sclerosing disease. Jpn J Ophthalmol. 2011. 55:315–317.5. Katsura M, Morita A, Horiuchi H, Ohtomo K, Machida T. IgG4-related inflammatory pseudotumor of the trigeminal nerve: another component of IgG4-related sclerosing disease? AJNR Am J Neuroradiol. 2011. 32:E150–E152.6. Park SB, Cho KS, Kim JK, Lee JH, Jeong AK, Kwon WJ, et al. Inflammatory pseudotumor (myoblastic tumor) of the genitourinary tract. AJR Am J Roentgenol. 2008. 191:1255–1262.7. Zen Y, Fujii T, Sato Y, Masuda S, Nakanuma Y. Pathological classification of hepatic inflammatory pseudotumor with respect to IgG4-related disease. Mod Pathol. 2007. 20:884–894.8. Yamamoto H, Yamaguchi H, Aishima S, Oda Y, Kohashi K, Oshiro Y, et al. Inflammatory myofibroblastic tumor versus IgG4-related sclerosing disease and inflammatory pseudotumor: a comparative clinicopathologic study. Am J Surg Pathol. 2009. 33:1330–1340.9. Narla LD, Newman B, Spottswood SS, Narla S, Kolli R. Inflammatory pseudotumor. Radiographics. 2003. 23:719–729.10. Harr DL, Quencer RM, Abrams GW. Computed tomography and ultrasound in the evaluation of orbital infection and pseudotumor. Radiology. 1982. 142:395–401.11. Andrich DE, Rickards D, Landon DN, Fowler CJ, Mundy AR. Structural assessment of the urethral sphincter in women with urinary retention. J Urol. 2005. 173:1246–1251.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Immunoglobulin G4-Related Sclerosing Disease Mimicking Lung Cancer
- Immunoglobulin G4-related sclerosing cholangitis
- Immunoglobulin G4-Related Systemic Sclerosing Disease: A Case Involving the Ureter and Kidney
- Two Cases of Immunoglobulin G4-Related Sclerosing Disease Mimicking Nasopharyngeal Carcinoma
- Poor positive predictive value of serum immunoglobulin G4 concentrations in the diagnosis of immunoglobulin G4-related sclerosing disease
