Antitumor Effect of in Situ Cryoablation with Systemic Immunotherapy on Murine Renal Cell Tumor
- Affiliations
-
- 1Department of Urology, College of Medicine, Korea University, Seoul, Korea. dkyoon@korea.ac.kr
- KMID: 1328166
- DOI: http://doi.org/10.4111/kju.2008.49.11.965
Abstract
-
PURPOSE: To investigate synergistic effect of local cryoablation with systemic immunotherapy, the tumor control ability and immunologic responses of combining these two modalities was compared with that of cryoablation, surgical excision, and immunotherapy only group in a tumor re-challenge model.
MATERIALS AND METHODS
Preliminary experiments were performed in two stages. The first stage consisted of 36 Balb/c mice with Renca bearing tumors imbedded in the right thigh, and was treated with interleukin-2 (IL-2) and interferon-alpha(IFN-alpha) to evaluate the efficacy of immunotherapy and to determine the adequate dosage. The second stage was performed on 10 mice, to evaluate histological changes and efficacy after cryoablation. The main experiment was performed on 48 mice, divided into 6 groups of control with tumor implantation, excision of tumor, excision combined with immunotherapy, cryoablation of tumor, cryoablation with immunotherapy and control without tumor. After treatment, tumor re-challenge was performed with Renca cell, then the growth pattern was evaluated with physical measurements, and immune response was investigated with fluorescent activated cell sorter and cytotoxicity assay.
RESULTS
Preliminary studies on immunologic efficacy revealed that IL-2 and IFN-alpha have a dose dependent inhibition of tumor growth. The main experiment evaluating the efficacy of combination treatment revealed that cryoablation with immunotherapy proved to be most effective in terms of tumor recurrence and tumor growth inhibition, yet the difference was not statistically significant from monotherapy with cryoablation. However, cytotoxicity was significantly increased cryoablation with immunotherapy compared with other groups.
CONCLUSIONS
Cryoablation on tumor re-challenge mice model showed advantages with immunotherapy most prominently in cytotoxicity.
Keyword
Figure
-
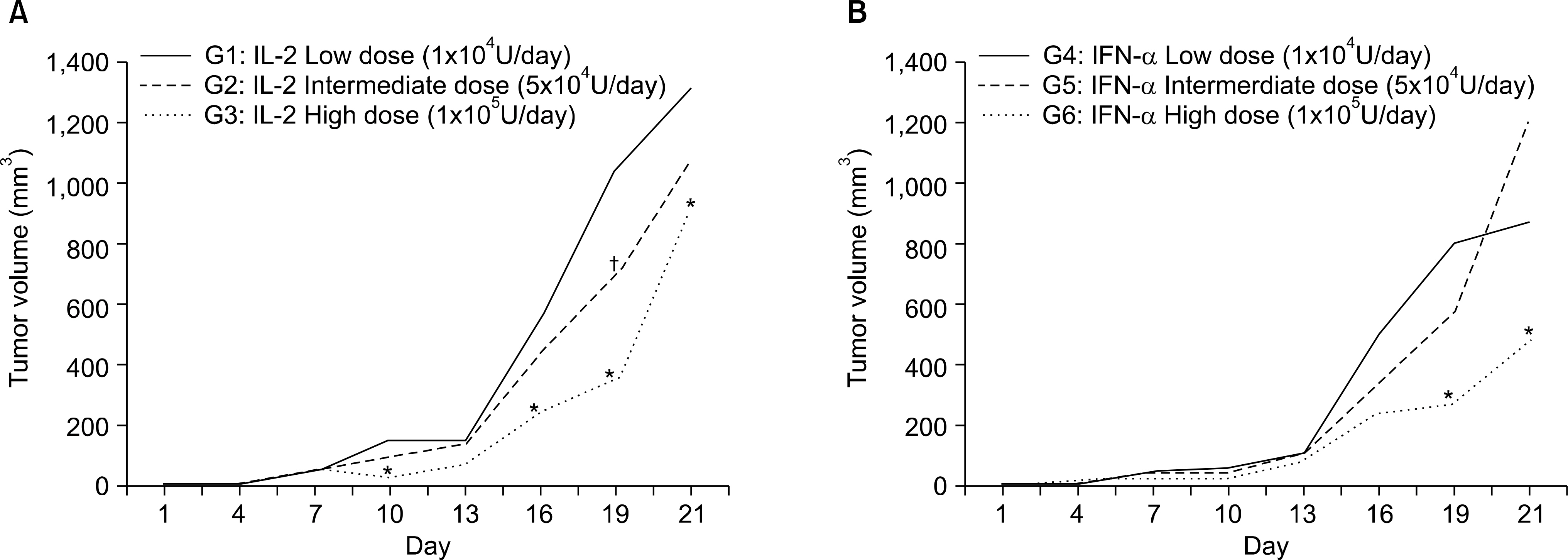
Fig. 1. Changes of the tumor volume in the preliminary studies to evaluate an adequate dose of the immunologic agents. (A) Changes of tumor volume in the IL-2 treated groups. (B) Changes of tumor volume in the IFN-α treated groups. ∗: significant difference of the tumor volume in the high dose administration group for each agent, as compared to the low dose administered group (p<0.05 by the Mann-Whitney U test). †: significant difference of the tumor volume of the intermediate dose administered group for each agent, as compared to the low dose administered group (p<0.05 by the Mann-Whitney U test). IL-2: interleukin-2, IFN-α: interferon-alpha.

Fig. 2. Results of the histologic examination, and the samples were taken at 2 days and 7 days after cryosurgery. Histologic change at (A-C) 2 days after cryoablation and (D-F) 7 days after cryoablation. (A) Central coagulative necrosis caused by cryoablation (H&E, x100). (B) At high magnification, shrunken and condensed cells with compact nuclei and pyknotic chromatin was found in the periphery of this zone, which are typical features of apoptosis (H&E, x200). (C) The areas of necrosis and apoptosis were surrounded by intact tumor cells, which were larger and they had slack chromatin (H&E, x200). (D) 7 days after the cryoablation was conducted, there was a wide area of necrosis without viable tumor cells (H&E, x40). (E) At high magnification, the central necrotic area was characterized by ghost cells and no apparent nuclei (H&E, x200). (F) This infiltration of neutrophils was a prominent finding at the peripheral muscular tissue, which was located below the previous injection site (H&E, x200).
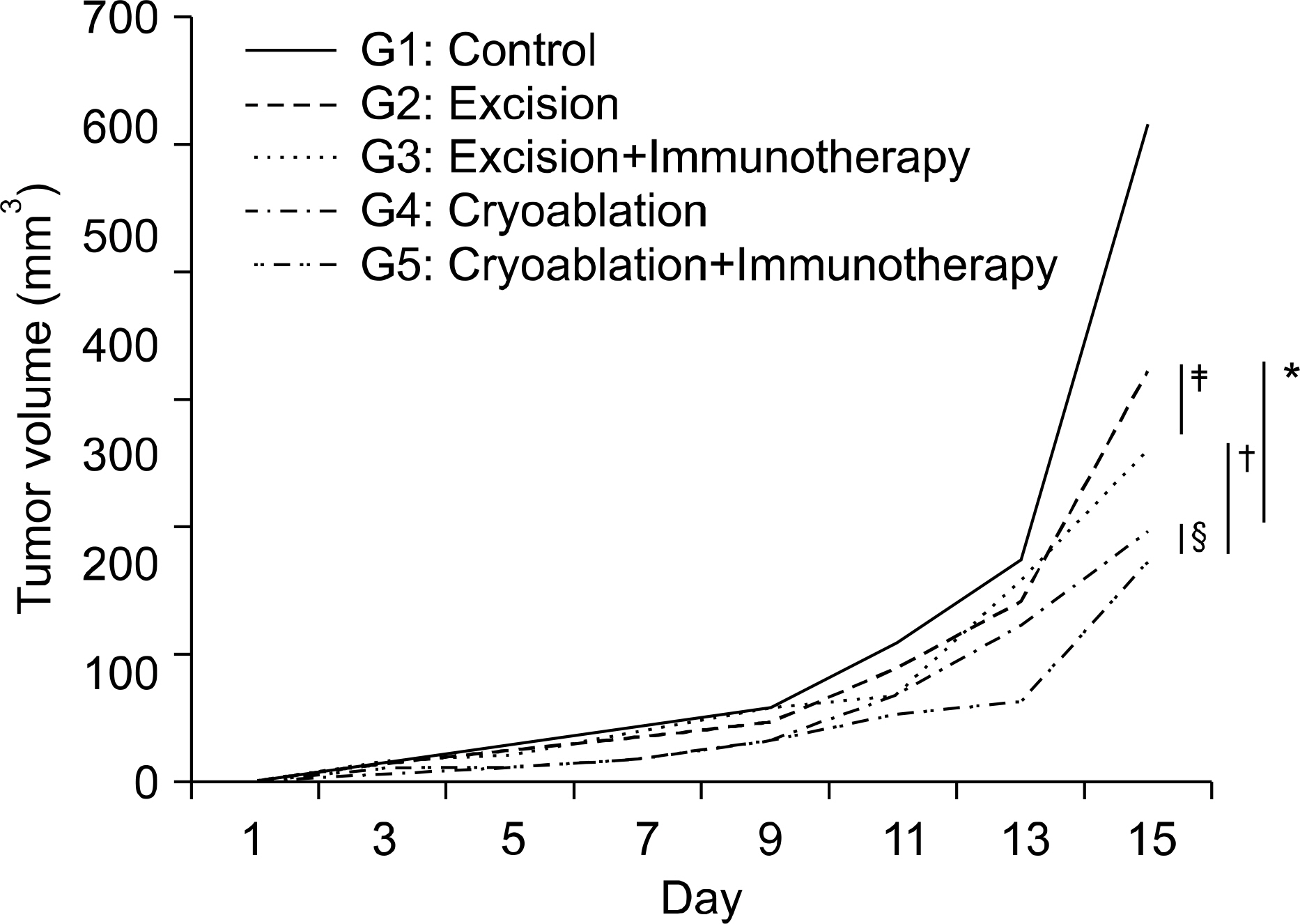
Fig. 3. The tumor growth pattern for each treatment after tumor re-challenge. At day 15, the tumor volume was significantly lower in the cryoablated group (G4, G5) than that in the surgical excised group of G2 and G3, respectively. ∗: significant decrease of the tumor volume in the cryoablation only group (G4), as compared to the excision only group (G2) (p=0.02, by the Mann-Whitney U test), †: significant decrease of tumor volume in the cryoablation with immunotherapy group (G5), as compared to the excision group plus immunotherapy group (G3) (p=0.04 by the Mann-Whitney U test), ‡: the difference of tumor volume in the excision with immunotherapy group (G3), as compared to the excision only group (G2), did not reach statistic significance (p=0.62 by the Mann-Whitney U test). §: the difference of tumor volume in the cryoablation with immunotherapy group (G5), as compared to the cryoablation group (G4) did not reach statistic significance (p=0.9 by the Mann-Whitney U test).

Fig. 4. Fluorescent activated cell sorter (FACS) results after tumor re-challenge. On comparison with the excision group, the percentages of gated CD4 and CD8 T cells of group 3, which was treated with surgical excision with immunotherapy, were significantly increased (∗: p=0.021 and 0.047 by the Mann-Whitney U test for the CD4 and CD8 cells, respectively). However, the difference between the cryoablation group and the combination group of cryoablation with immunotherapy did not reach a significant value (†: p=0.19 for CD4, below 0.05 for the other cytokines).
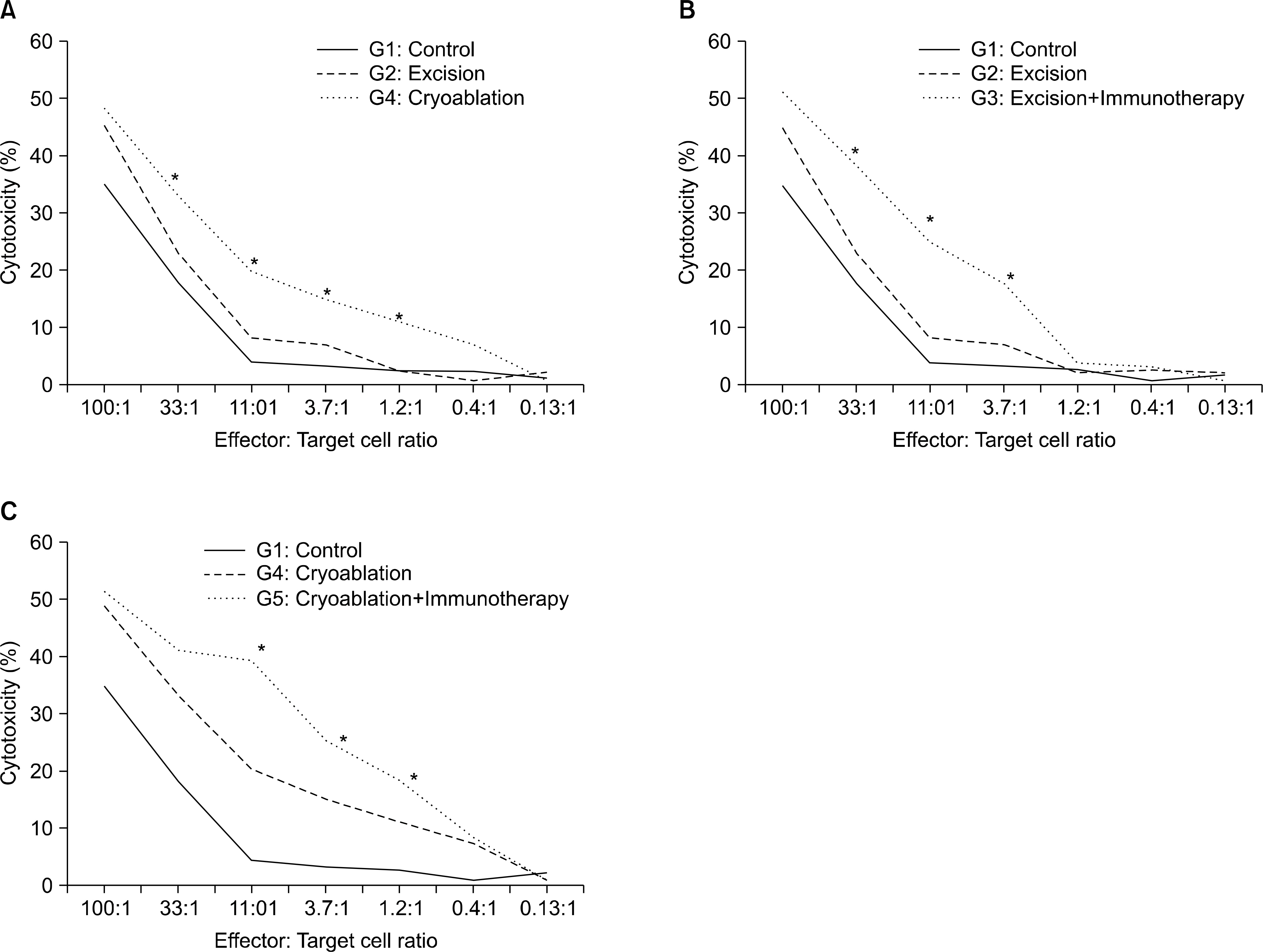
Fig. 5. Result of the cytotoxicity assay, after tumor re-challenge. (A) The cryoablation group showed increased cytotoxicity at effector: the target cell ratios were 33:1, 11:1, 3.7:1 and 1.2:1, respectively. ∗: significantly increased compared to the excision group (p<0.05, by the Mann-Whitney U test). (B) The excision with immunotherapy group showed increased cytotoxicity at effector: the target cell ratios were 33:1, 11:1 and 3.7:1, respectively ∗: significant increased compared to the excision only group (p<0.05, by the Mann-Whitney U test). (C) The cryoablation group with immunotherapy group showed increased cytotoxicity at effector: the target cell ratios were 11:1, 3.7:1 and 1.2:1, respectively. ∗: significant increased compared with the cryoablation only group (p<0.05, by the Mann-Whitney U test).
Reference
-
References
1. Flanigan RC. Debulking nephrectomy in metastatic renal cancer. Clin Cancer Res. 2004; 10:S6335–41.
Article2. Jacobs SC, Berg SI, Lawson RK. Synchronous bilateral renal cell carcinoma: total surgical excision. Cancer. 1980; 46:2341–5.
Article3. Moll V, Becht E, Ziegler M. Kidney preserving surgery in renal cell tumors: indications, techniques and results in 152 patients. J Urol. 1993; 150:319–23.
Article4. Belldegrun A, Tsui KH, deKernion JB, Smith RB. Efficacy of nephron-sparing surgery for renal cell carcinoma: analysis based on the new 1997 tumor-node-metastasis staging system. J Clin Oncol. 1999; 17:2868–75.
Article5. Patard JJ, Kim HL, Lam JS, Dorey FJ, Pantuck AJ, Zisman A, et al. Use of the University of California Los Angeles integrated staging system to predict survival in renal call carcinoma: an international multicenter study. J Clin Oncol. 2004; 22:3316–22.6. Campbell SC, Novick AC, Bukowski RM. Renal tumors. Kavoussi LR, Novick AC, Partin AW, Peters CA, Wein AJ, editors. editors.Campbell's urology. 9th ed.Philadelphia: Saunders;2007. p. 1567–637.7. Colimbu M, Joshi P, Sperber A, Tessler A, Al-Askari S, Morales P. Renal cell carcinoma: survival and prognostic factors. Urology. 1986; 27:291–301.
Article8. Hafez KS, Montie JE. Indication and limitations of cytoreductive nephrectomy for metastatic renal cell carcinoma. AUA Update Series. 2004. ;lesson 31.9. O'Malley RL, Berger AD, Kanofsky JA, Phillips CK, Stifel-man M, Taneja SS. A matched-cohort comparison of laparoscopic cryoablation and laparoscopic partial nephrectomy for treating renal masses. BJU Int. 2007; 99:395–8.10. Hruby G, Reisiger K, Venkatesh R, Yan Y, Landman J. Comparison of laparoscopic partial nephrectomy and laparoscopic cryoablation for renal hilar tumors. Urology. 2006; 67:50–4.
Article11. Ablin RJ. An appreciation and realization of the concept of cryoimmunology. Ablin RJ, editor. Percutaneous prostate cryoablation. 1st ed.St. Louis: Quality Medical Publishing;1995. p. 136–54.12. Suzuki Y. Cryosurgical treatment of advanced breast cancer and cryoimmunological responses. Skin Cancer. 1995; 10:19–26.13. Hornung RL, Back TC, Zaharko DS, Urba WJ, Longo DL, Wiltrout RH. Augmentation of natural killer activity, induction of IFN and development tumor immunity during the successful treatment of established murine renal cancer using flavone acetic acid and IL-2. J Immunol. 1988; 141:3671–9.14. Sayers TJ, Wiltrout TA, McCormick K, Husted C, Wiltrout RH. Antitumor effects of alpha-interferon and gamma-interferon on a murine renal cancer (Renca) in vitro and in vivo. Cancer Res. 1990; 50:5414–20.15. Fergany AF, Hafez KS, Novick AC. Long-term results of nephron sparing surgery for localized renal cell carcinoma: 10-year follow up. J Urol. 2000; 163:442–5.16. Gage AA, Huben R. Cryosurgical ablation of the prostate. Urol Oncol. 2000; 5:19–24.
Article17. Sabel MS, Edge SB. In-situ ablation of breast cancer. Breast Dis. 2001; 12:131–40.
Article18. Johnson JP. Immunologic aspects of cryosurgery: potential modulation of immune recognition and effector cell maturation. Clin Dermatol. 1990; 8:39–47.
Article19. Sabel M, Arora A, Su G, Chang AE. Adoptive immunotherapy of breat cancer with lymph node cells primed by cryoablation of the primary tumor. Cryobiology. 2006; 53:360–6.20. Ablin RJ, Jagodzinski RV, Prox C, Williams RW, Gonder MJ, Soanes WA. Cryosurgery of the monkey (macaque) prostate. I. Humoral immunologic responsiveness following cryosti-mulation. Cryobiology. 1976; 13:47–53.21. Airoldi M, Fazio M, Gandolfo S, Ozzello F, Pedani F, Brando V, et al. Combined chemotherapy, cryosurgery, and radiotherapy/surgery for oral cancer. Int J Clin Pharmacol Res. 1985; 5:357–62.22. Fujikawa S, Suzuki T, Ishikawa T, Sakurai S, Hasegawa Y. Continuous observation of frozen biological materials with cryo-scanning electron microscope and freeze-replica by a new cryo-system. J Electron Microsc. 1988; 37:315–22.23. Kang SH, Bae JH, Shim KS. The development of tumour-specific immunity induced by cryosurgery in murine renal cell carcinoma animal model. Eur Urol. 2006; 5(Suppl):): 29.
Article24. Kaouk JH, Aron M, Rewcastle JC, Gill IS. Cryotherapy: clinical end points and their experimental foundations. Urology. 2006; 68(1 Suppl):38–44.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anti-tumor Immune Response after Cryoablation in Renal Cell Carcinoma Murine Model
- Effect of BCG Immunotherapy on the Cytokine Production and Antitumor Activity against MBT - 2 Mouse Bladder Tumor
- Immunologic Response to Cryoablation of Squamous Cell Carcinoma
- Urologic Applications of Cryo-Immunology
- The Initial Experience with 3rd Generation Nephron-sparing Cryoablation for Renal Tumor
