Korean J Transplant.
2022 Dec;36(4):278-282. 10.4285/kjt.22.0026.
Newly diagnosed metastatic pulmonary calcification in a kidney transplantation recipient: a case report
- Affiliations
-
- 1Division of Nephrology, Department of Internal Medicine, Eunpyeong St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Transplantation Research Center, Division of Nephrology, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 3Convergent Research Consortium for Immunologic Disease, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2537539
- DOI: http://doi.org/10.4285/kjt.22.0026
Abstract
- Metastatic pulmonary calcification (MPC) is defined as calcium deposition in lung tissues. It is commonly seen in end-stage renal disease patients. However, MPC occurring in kidney transplant recipients (KTRs) is rare. We report a case of MPC in a 55-year-old female patient after successful kidney transplantation (KT). One year after KT, bisphosphonate and vitamin D were prescribed for osteoporosis. Then, 4.5 years after KT, we incidentally found multiple nodular lesions on chest X-ray (CXR) without any symptoms. Chest computed tomography showed multiple high-density nodules. A bone scan confirmed MPC in the right middle lobe and right lower lobe. A retrospective review of pretransplant blood chemistry revealed the following: serum calcium level, 11.2 mg/dL; phosphorus level, 3.2 mg/dL; intact parathyroid hormone level, lower than 2.5 pg/mL; and 24-hour urine calcium level, within normal limits (WNL). After KT, all of these parameters remained WNL. Therefore, hidden adynamic bone disease might have been aggravated by bisphosphonate and vitamin D supplementation, causing MPC. Both were discontinued. She was monitored by routine CXR, and MPC did not progress. Since MPC is commonly asymptomatic and difficult to diagnose in KTRs, caution is required when administering such medications. Patient should be followed up with routine CXR.
Figure
-
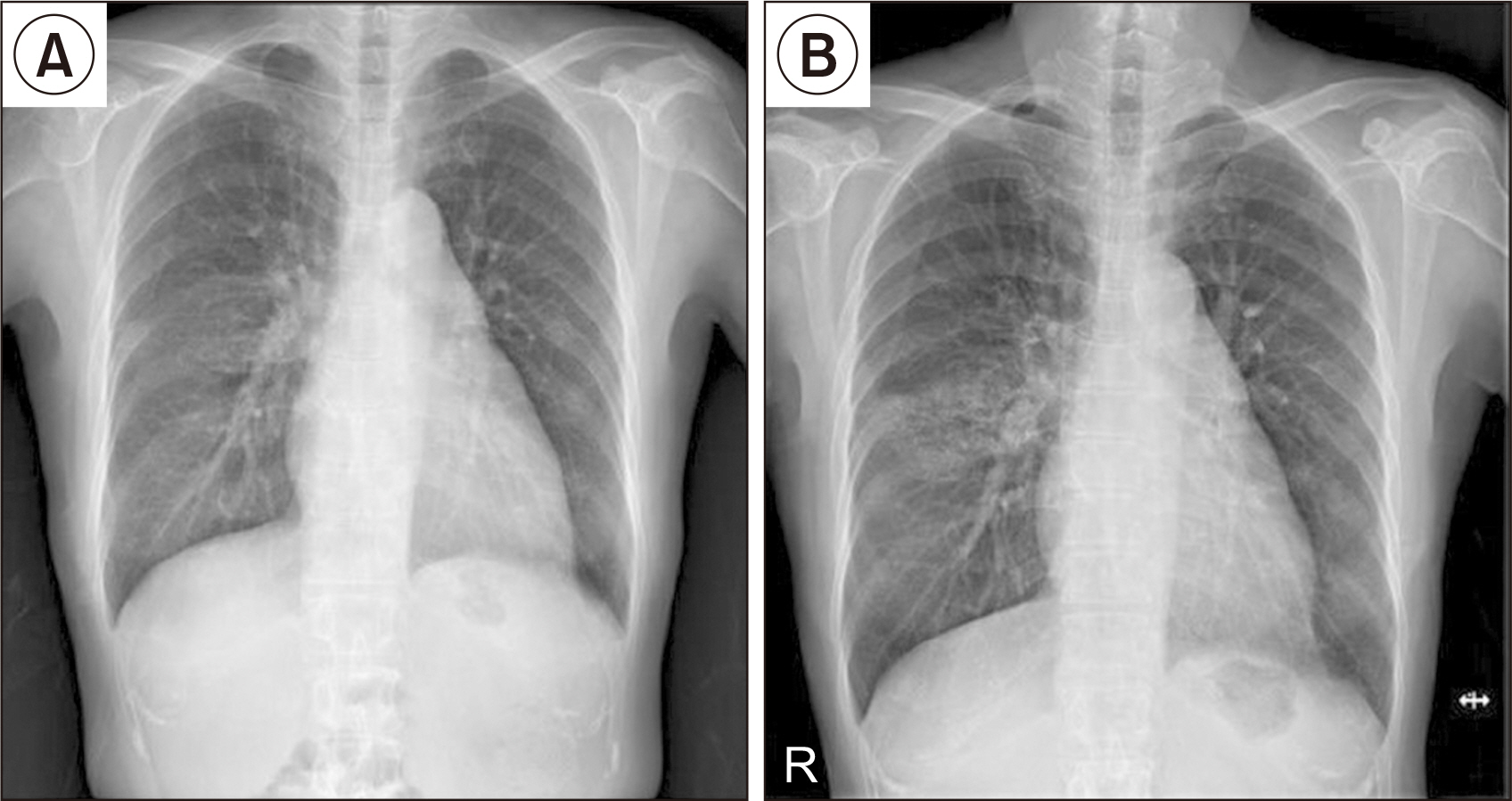
Fig. 1 Chest X-ray (CXR) of the patient. (A) CXR taken 1 year after kidney transplantation (KT) shows no abnormal findings. (B) CXR taken 4.5 years after KT shows metastatic pulmonary calcification in the right middle lobe.
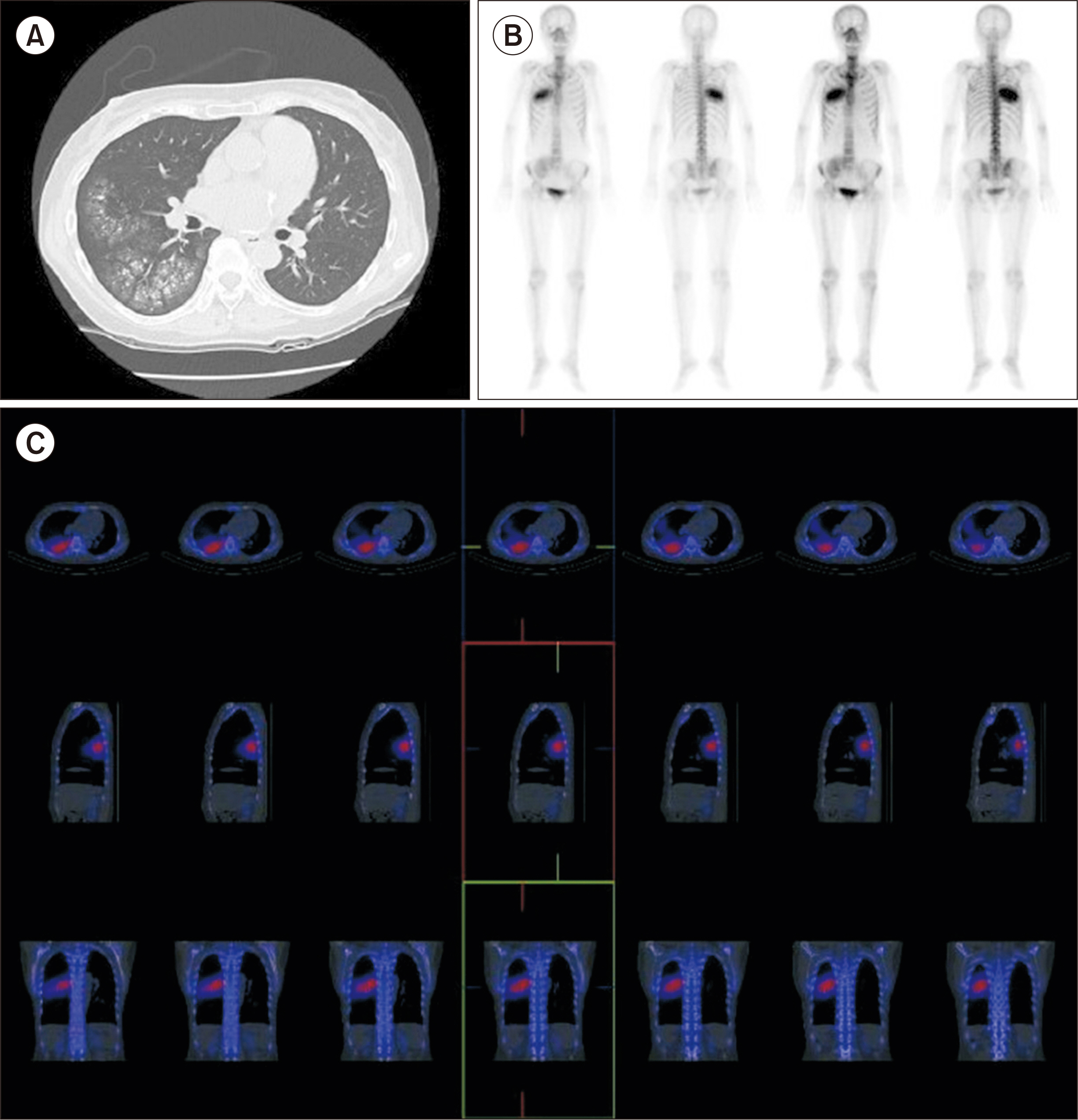
Fig. 2 (A) Low-dose chest computed tomography of the patient shows multiple centrilobular nodules in the right middle lobe (RML) and right lower lobe (RLL). (B, C) A bone scan confirmed metastatic pulmonary calcification in the RML and RLL.
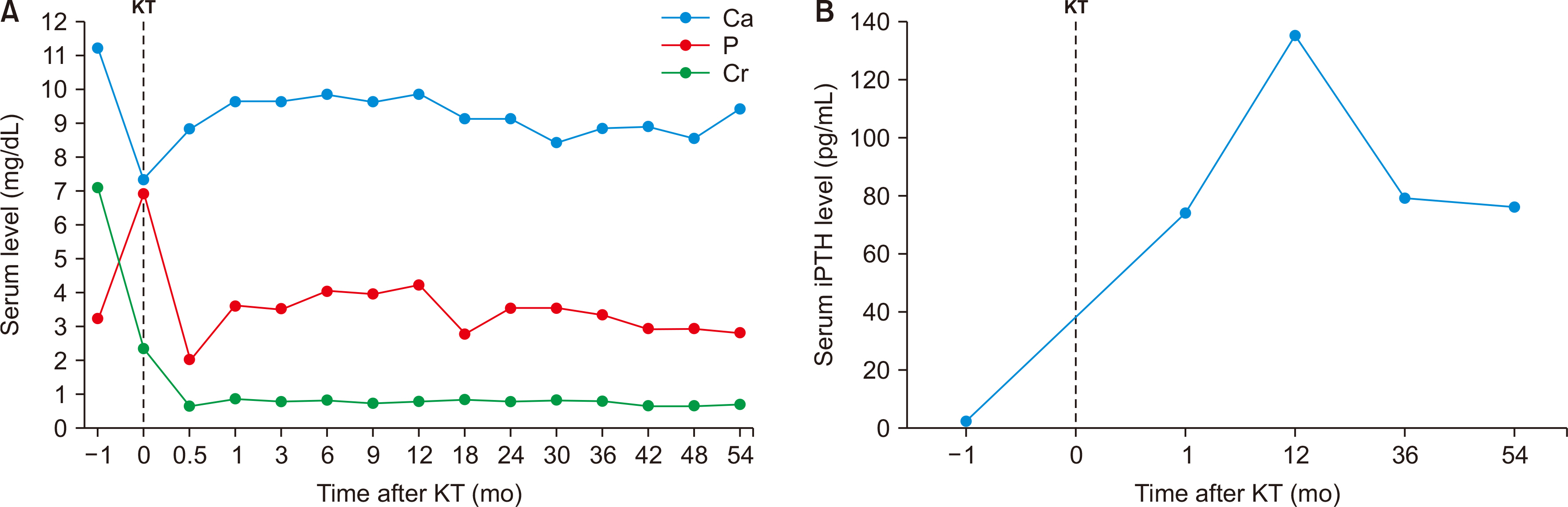
Fig. 3 Summary of changes in laboratory findings over time after kidney transplantation (KT; months). (A) Changes in serum calcium (Ca), phosphorus (P), and creatinine (Cr) levels. (B) Changes in intact parathyroid hormone (iPTH) level.
Reference
-
1. Chan ED, Morales DV, Welsh CH, McDermott MT, Schwarz MI. 2002; Calcium deposition with or without bone formation in the lung. Am J Respir Crit Care Med. 165:1654–69. DOI: 10.1164/rccm.2108054. PMID: 12070068.2. Davies MR, Hruska KA. 2001; Pathophysiological mechanisms of vascular calcification in end-stage renal disease. Kidney Int. 60:472–9. DOI: 10.1046/j.1523-1755.2001.060002472.x. PMID: 11473629.3. Kuzela DC, Huffer WE, Conger JD, Winter SD, Hammond WS. 1977; Soft tissue calcification in chronic dialysis patients. Am J Pathol. 86:403–24. PMID: 836675. PMCID: PMC2032079.4. Sun HM, Chen F, Yin HL, Xu XY, Liu HB, Zhao BL. 2017; Rapid development of metastatic pulmonary calcifications in primary hyperparathyroidism: a case report and literature review. Diagn Pathol. 12:38. DOI: 10.1186/s13000-017-0628-1. PMID: 28482911. PMCID: PMC5423015.5. Katzenstein AA, Askin FB. 1982; Surgical pathology of non-neoplastic lung disease. Major Probl Pathol. 13:1–430. DOI: 10.1038/modpathol.3880056. PMID: 7087547.6. Wesseling-Perry K, Bacchetta J. 2011; CKD-MBD after kidney transplantation. Pediatr Nephrol. 26:2143–51. DOI: 10.1007/s00467-011-1829-6. PMID: 21394466. PMCID: PMC3203246.7. Thurley PD, Duerden R, Roe S, Pointon K. 2009; Case report: rapidly progressive metastatic pulmonary calcification: evolution of changes on CT. Br J Radiol. 82:e155–9. DOI: 10.1259/bjr/87606661. PMID: 19592398.8. Guermazi A, Espérou H, Selimi F, Gluckman E. 2005; Imaging of diffuse metastatic and dystrophic pulmonary calcification in children after haematopoietic stem cell transplantation. Br J Radiol. 78:708–13. DOI: 10.1259/bjr/74299224. PMID: 16046422.9. Faubert PF, Shapiro WB, Porush JG, Chou SY, Gross JM, Bondi E, et al. 1980; Pulmonary calcification in hemodialyzed patients detected by technetium-99m diphosphonate scanning. Kidney Int. 18:95–102. DOI: 10.1038/ki.1980.114. PMID: 7218663.10. Brandenburg VM, Floege J. 2008; Adynamic bone disease-bone and beyond. NDT Plus. 1:135–47. DOI: 10.1093/ndtplus/sfn040. PMID: 25983860. PMCID: PMC4421169.11. Sprague SM. 2000; The role of the bone biopsy in the diagnosis of renal osteodystrophy. Semin Dial. 13:152–5. DOI: 10.1046/j.1525-139x.2000.00042.x. PMID: 10833774.12. Amerling R, Harbord NB, Pullman J, Feinfeld DA. 2010; Bisphosphonate use in chronic kidney disease: association with adynamic bone disease in a bone histology series. Blood Purif. 29:293–9. DOI: 10.1159/000276666. PMID: 20090316.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Metastatic pulmonalry calcification associated with malignant lymphoma: a case report
- Mandibular Enlargement, Metastatic Pulmonary Calcification and Gastric Mucosal Calcinosis in a Patient with Chronic Kidney Disease-mineral Bone Disorder
- Transplantation of En Bloc Pediatric Cadaver Kidneys into Adult Recipient
- A Case of Metastatic Gastric Calcification in Acute Renal Failure
- Metastatic Calcification of the Finger in a Chronic Renal Failure Patient
