Clin Endosc.
2022 Nov;55(6):793-800. 10.5946/ce.2021.211.
A prospective study of fully covered self-expandable metal stents for refractory benign pancreatic duct strictures
- Affiliations
-
- 1Institute of Gastrosciences & Liver, Apollo Multispeciality Hospital, Kolkata, India
- 2Department of Clinical Imaging and Interventional Radiology, Apollo Gleneagles Hospital, Kolkata, India
- KMID: 2536080
- DOI: http://doi.org/10.5946/ce.2021.211
Abstract
- Background/Aims
Fully covered self-expanding metal stents (FCSEMSs) are a relatively novel option for treating painful main pancreatic duct refractory strictures in patients with chronic pancreatitis. Herein, we aimed to assess the efficacy, feasibility, and safety of FCSEMSs in this patient group.
Methods
This prospective single-center study included patients who underwent endoscopic retrograde pancreatography with FCSEMS placement. The primary endpoints were the technical and clinical success rates. A reduction in visual analog scale pain score of >50% compared with that before stent placement was defined as clinical success. Secondary endpoints were resolution of pancreatic strictures on fluoroscopy during endoscopic retrograde pancreatography and the development of stent-related adverse events.
Results
Thirty-six patients were included in the analysis. The technical success rate was 100% (n=36) and the clinical success rate was 86.1% (n=31). There was a significant increase in stricture diameter from 1.7 mm to 3.5 mm (p<0.001) after stent removal. The mean visual analog scale pain score showed statistically significant improvement. At 19 months of follow-up, 55.6% of the patients were asymptomatic. Stent migration (16.7%), intolerable abdominal pain (8.3%), development of de novo strictures (8.3%), and mild pancreatitis (2.8%) were the most common adverse events.
Conclusions
FCSEMS placement showed good technical and clinical success rates for achieving pain relief in patients with refractory main pancreatic duct strictures.
Keyword
Figure
-

Fig. 1. (A) Pancreatogram obtained before placement of the metal stent showing a tight stricture in the head of the pancreatic duct. (B) Dilatation of pancreatic duct stricture by the hydrostatic balloon. (C) Pancreatogram after Niti-S [Bumpy] stent deployment. (D) Follow-up pancreatogram at 3 months showing resolution of the pancreatic duct stricture.
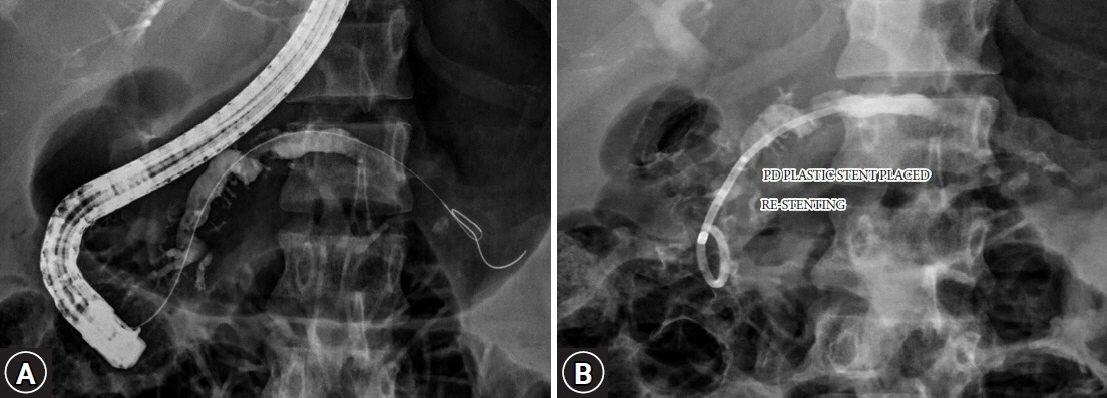
Fig. 2. (A) Occurrence of a de novo pancreatic duct stricture after stent removal. (B) Placement of a plastic pancreatic duct stent across the stricture.
Reference
-
1. Goulden MR. The pain of chronic pancreatitis: a persistent clinical challenge. Br J Pain. 2013; 7:8–22.
Article2. Rösch T, Daniel S, Scholz M, et al. Endoscopic treatment of chronic pancreatitis: a multicenter study of 1000 patients with long-term follow-up. Endoscopy. 2002; 34:765–771.
Article3. Gabbrielli A, Pandolfi M, Mutignani M, et al. Efficacy of main pancreatic-duct endoscopic drainage in patients with chronic pancreatitis, continuous pain, and dilated duct. Gastrointest Endosc. 2005; 61:576–581.
Article4. Dumonceau JM, Delhaye M, Tringali A, et al. Endoscopic treatment of chronic pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) guideline - updated August 2018. Endoscopy. 2019; 51:179–193.
Article5. Cremer M, Devière J, Delhaye M, et al. Stenting in severe chronic pancreatitis: results of medium-term follow-up in seventy-six patients. Bildgebung. 1992; 59(Suppl 1):20–24.
Article6. Smits ME, Badiga SM, Rauws EA, et al. Long-term results of pancreatic stents in chronic pancreatitis. Gastrointest Endosc. 1995; 42:461–467.
Article7. Binmoeller KF, Jue P, Seifert H, et al. Endoscopic pancreatic stent drainage in chronic pancreatitis and a dominant stricture: long-term results. Endoscopy. 1995; 27:638–644.
Article8. Shen Y, Liu M, Chen M, et al. Covered metal stent or multiple plastic stents for refractory pancreatic ductal strictures in chronic pancreatitis: a systematic review. Pancreatology. 2014; 14:87–90.
Article9. Ponchon T, Bory RM, Hedelius F, et al. Endoscopic stenting for pain relief in chronic pancreatitis: results of a standardized protocol. Gastrointest Endosc. 1995; 42:452–456.
Article10. Delhaye M, Arvanitakis M, Verset G, et al. Longterm clinical outcome after endoscopic pancreatic ductal drainage for patients with painful chronic pancreatitis. Clin Gastroenterol Hepatol. 2004; 2:1096–1106.
Article11. Eleftherladis N, Dinu F, Delhaye M, et al. Long-term outcome after pancreatic stenting in severe chronic pancreatitis. Endoscopy. 2005; 37:223–230.
Article12. Weber A, Schneider J, Neu B, et al. Endoscopic stent therapy for patients with chronic pancreatitis: results from a prospective follow-up study. Pancreas. 2007; 34:287–294.13. Costamagna G, Bulajic M, Tringali A, et al. Multiple stenting of refractory pancreatic duct strictures in severe chronic pancreatitis: long-term results. Endoscopy. 2006; 38:254–259.14. Tringali A, Vadalà di Prampero SF, et al. Fully covered self-expandable metal stents to dilate persistent pancreatic strictures in chronic pancreatitis: long-term follow-up from a prospective study. Gastrointest Endosc. 2018; 88:939–946.
Article15. Park DH, Kim MH, Moon SH, et al. Feasibility and safety of placement of a newly designed, fully covered self-expandable metal stent for refractory benign pancreatic ductal strictures: a pilot study (with video). Gastrointest Endosc. 2008; 68:1182–1189.
Article16. Moon SH, Kim MH, Park DH, et al. Modified fully covered self-expandable metal stents with antimigration features for benign pancreatic-duct strictures in advanced chronic pancreatitis, with a focus on the safety profile and reducing migration. Gastrointest Endosc. 2010; 72:86–91.
Article17. Matsubara S, Sasahira N, Isayama H, et al. Prospective pilot study of fully covered self-expandable metal stents for refractory benign pancreatic duct strictures: long-term outcomes. Endosc Int Open. 2016; 4:E1215–E1222.
Article18. Lee YN, Moon JH, Park JK, et al. Preliminary study of a modified, nonflared, short, fully covered metal stent for refractory benign pancreatic duct strictures (with videos). Gastrointest Endosc. 2020; 91:826–833.
Article19. Dumonceau JM. Endoscopic therapy for chronic pancreatitis. Gastrointest Endosc Clin N Am. 2013; 23:821–832.
Article20. Jafri M, Sachdev A, Sadiq J, et al. Efficacy of endotherapy in the treatment of pain associated with chronic pancreatitis: a systematic review and meta-analysis. JOP. 2017; 18:125–132.21. Hirota M, Asakura T, Kanno A, et al. Long-period pancreatic stenting for painful chronic calcified pancreatitis required higher medical costs and frequent hospitalizations compared with surgery. Pancreas. 2011; 40:946–950.
Article22. Sauer B, Talreja J, Ellen K, et al. Temporary placement of a fully covered self-expandable metal stent in the pancreatic duct for management of symptomatic refractory chronic pancreatitis: preliminary data (with videos). Gastrointest Endosc. 2008; 68:1173–1178.
Article23. Giacino C, Grandval P, Laugier R. Fully covered self-expanding metal stents for refractory pancreatic duct strictures in chronic pancreatitis. Endoscopy. 2012; 44:874–877.
Article24. Ogura T, Onda S, Takagi W, et al. Placement of a 6 mm, fully covered metal stent for main pancreatic head duct stricture due to chronic pancreatitis: a pilot study (with video). Therap Adv Gastroenterol. 2016; 9:722–728.
Article25. Li TT, Song SL, Xiao LN, et al. Efficacy of fully covered self-expandable metal stents for the management of pancreatic duct strictures in chronic pancreatitis: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2020; 35:1099–1106.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of Benign and Malignant Pancreatic Duct Strictures
- Role of Fully Covered Self-Expandable Metal Stent for Treatment of Benign Biliary Strictures and Bile Leaks
- The Efficacy and Safety of Fully Covered Self-expandable Metal Stents in Benign Extrahepatic Biliary Strictures
- Refractory benign biliary stricture due to chronic pancreatitis in two patients treated using endoscopic ultrasound-guided choledochoduodenostomy fistula creation: case reports
- Temporary Placement of a Newly Designed, Fully Covered, Self-Expandable Metal Stent for Refractory Bile Leaks
