Duodenal Stricture due to Necrotizing Pancreatitis following Endoscopic Ultrasound-Guided Ethanol Ablation of a Pancreatic Cyst: A Case Report
- Affiliations
-
- 1Department of Internal Medicine and Liver Research Institute, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. gidoctor@snuh.org
- KMID: 2464675
- DOI: http://doi.org/10.5946/ce.2018.191
Abstract
- The frequency of incidental detection of pancreatic cystic lesions (PCLs) is increasing because of the frequent use of cross-sectional imaging. The appropriate treatment for PCLs is challenging, and endoscopic ultrasound-guided ablation for PCLs has been reported in several studies. Although the feasibility and efficacy of this therapeutic modality have been shown, the safety issues associated with the procedure are still a concern. We present a case of a 61-year-old man who underwent ultrasound-guided ethanol ablation for PCL and needed repeated endoscopic balloon dilatation for severe duodenal stricture caused by necrotizing pancreatitis after the cyst ablation therapy.
MeSH Terms
Figure
-
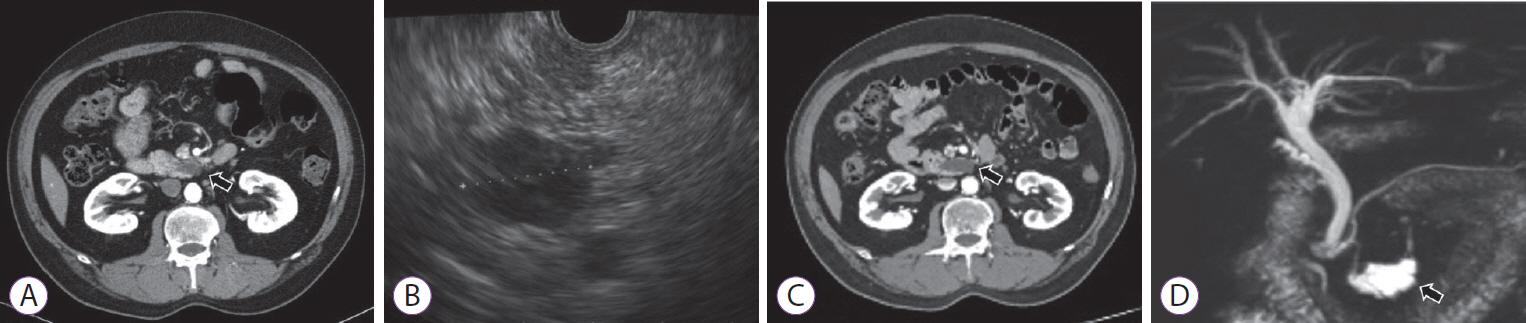
Fig. 1. Imaging evaluations of pancreatic cyst lesion. (A) Initial computed tomography (CT) scan revealed a 2.2-cm branch duct-intraductal papillary mucinous neoplasm in the uncinate process of the pancreas (arrow); (B) Initial endoscopic ultrasonography findings indicated a 2-cm unilocular cyst in the uncinate process without a definite mural nodule or pancreatic duct dilatation; (C) A follow-up CT showed a 3.5-cm cystic lesion with exophytic portion in the uncinate process, increased in size (arrow); (D) Magnetic resonance cholangiopancreatography revealed a 3.6-cm pleomorphic cystic lesion in the pancreas head with pancreatic duct communication and without main pancreatic duct dilatation or solid mural nodule (arrow).
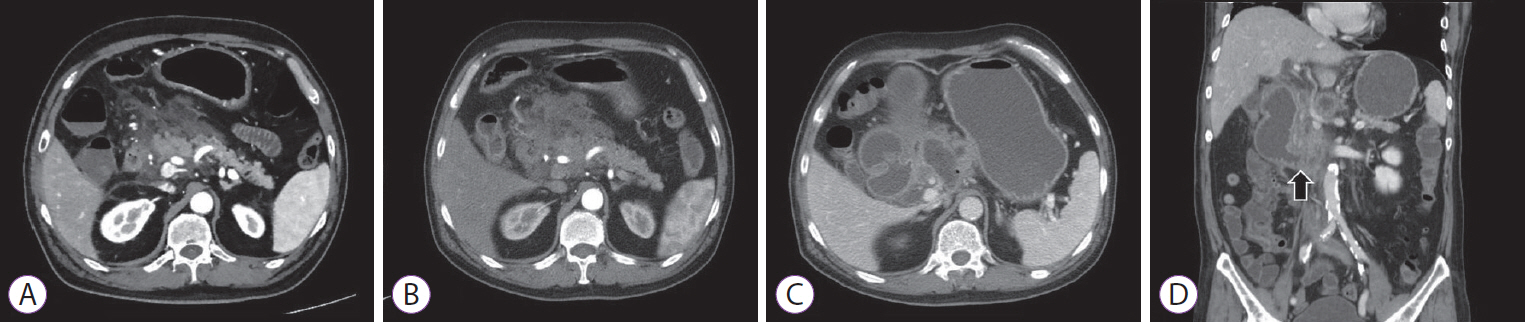
Fig. 2. Abdominal computed tomography (CT) findings. (A) Pancreatic swelling with extensive peripancreatic infiltration and fluid collection suggesting acute interstitial edematous pancreatitis; (B) Hypoenhancement of the pancreas with extensive areas of necrosis showing necrotizing pancreatitis; (C) A follow-up CT after 6 weeks revealed walled-off pancreatic necrosis; (D) Third duodenal portion narrowing (arrow) associated with upstream dilatation of the duodenum and stomach, suggesting gastric outlet obstruction.
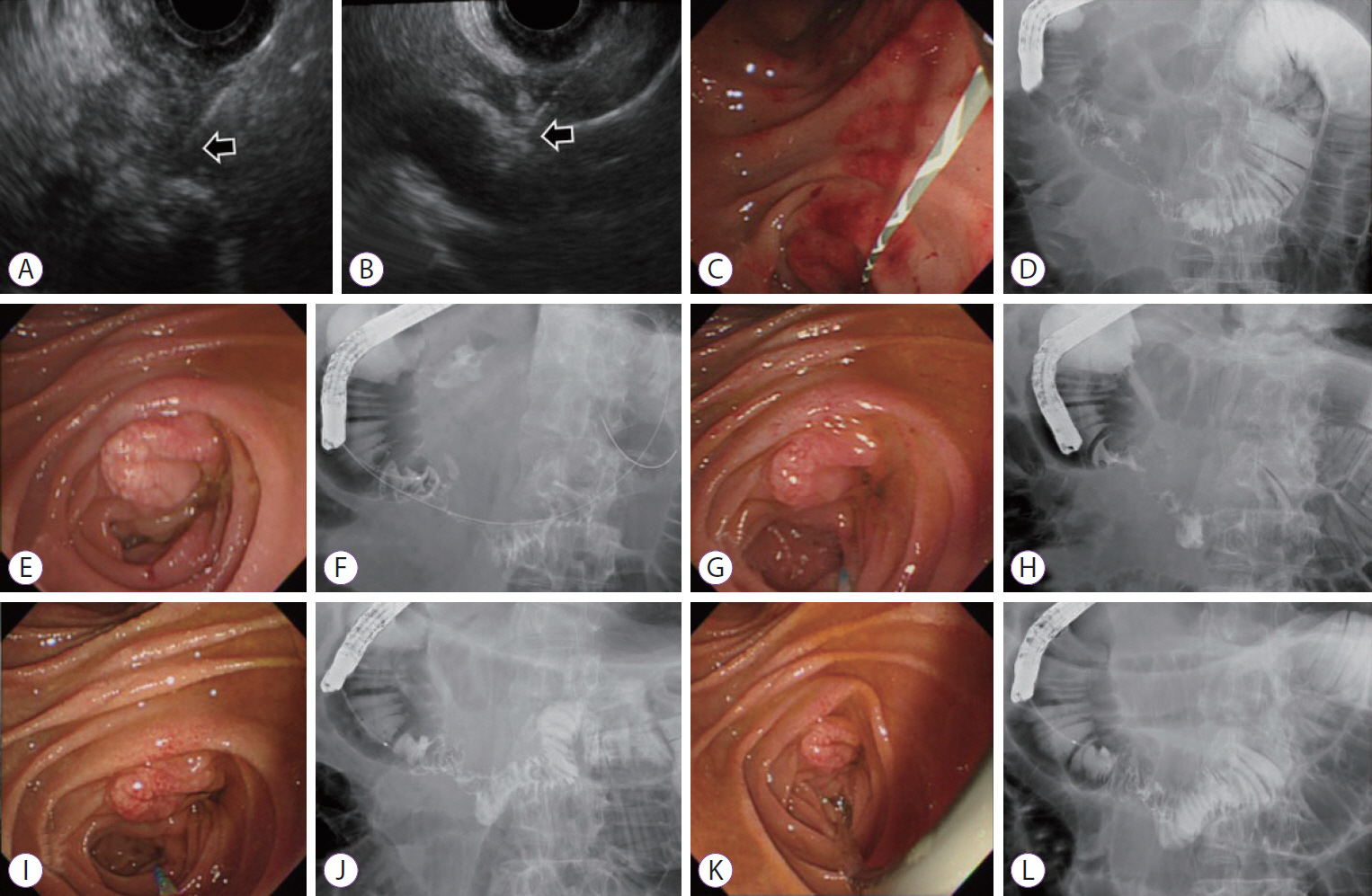
Fig. 3. Endoscopic balloon dilation (EBD) of the duodenal stricture. (A) Endoscopic ultrasonography (EUS) showing peripancreatic necrosis and aspiration attempts (arrow); (B) Part of walled-off necrosis was drained by EUS-guided aspiration using 19-gauge needle (arrow); (C) The stricture observed in the second part of the duodenum was not passed by the duodenoscope. The guidewire was passed to the third portion and EBD with the diameter of 20 mm was performed.; (D) The fluoroscopy showing dye passed through the third portion of duodenum, but not adequate. (E) After one week from first EBD, luminal narrowing was found in the second and third portions of the duodenum. (F) The second EBD was attempted. (G) Duodenoscope passage was still difficult due to narrowed lumen after a week. (H) Dye passage was confirmed after third EBD. (I, J) The fourth EBD was performed 3 times for 3 minutes, and the stricture was alleviated. (K, L) The improved state of stricture was confirmed after the 5th EBD.
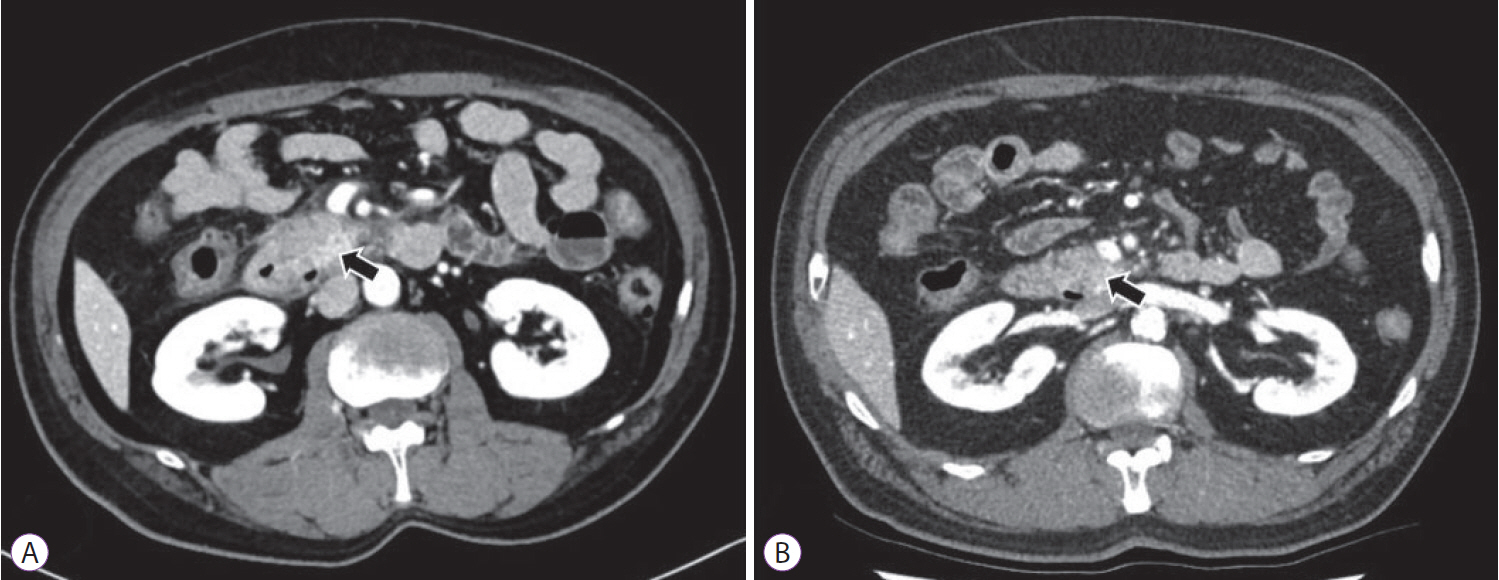
Fig. 4. Computed tomography (CT) images after resolution of procedure-related adverse events. (A) Abdominal CT scan performed 1 month after the last discharge, showed interval regression of pancreatitis and no duodenal obstruction (arrow); (B) Complete remission of pancreatic cystic lesion was revealed by the follow-up CT scan performed 9 months after cyst ablation (arrow).
Reference
-
1. Basar O, Brugge WR. My treatment approach: pancreatic cysts. Mayo Clin Proc. 2017; 92:1519–1531.
Article2. Lee SH. [Endoscopic treatment for pancreatic cystic lesions]. Korean J Gastroenterol. 2018; 71:10–17.
Article3. Park JK, Song BJ, Ryu JK, et al. Clinical outcomes of endoscopic ultrasonography-guided pancreatic cyst ablation. Pancreas. 2016; 45:889–894.
Article4. Tanaka M, Fernández-Del Castillo C, Kamisawa T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology. 2017; 17:738–753.
Article5. Allen PJ. The diagnosis and management of cystic lesions of the pancreas. Chin Clin Oncol. 2017; 6:60.
Article6. Gan SI, Thompson CC, Lauwers GY, Bounds BC, Brugge WR. Ethanol lavage of pancreatic cystic lesions: initial pilot study. Gastrointest Endosc. 2005; 61:746–752.
Article7. Oh HC, Seo DW, Lee TY, et al. New treatment for cystic tumors of the pancreas: EUS-guided ethanol lavage with paclitaxel injection. Gastrointest Endosc. 2008; 67:636–642.
Article8. Oh HC, Seo DW, Kim SC, et al. Septated cystic tumors of the pancreas: is it possible to treat them by endoscopic ultrasonography-guided intervention? Scand J Gastroenterol. 2009; 44:242–247.
Article9. DeWitt J, McGreevy K, Schmidt CM, Brugge WR. EUS-guided ethanol versus saline solution lavage for pancreatic cysts: a randomized, double-blind study. Gastrointest Endosc. 2009; 70:710–723.
Article10. Oh HC, Seo DW, Song TJ, et al. Endoscopic ultrasonography-guided ethanol lavage with paclitaxel injection treats patients with pancreatic cysts. Gastroenterology. 2011; 140:172–179.
Article11. DiMaio CJ, DeWitt JM, Brugge WR. Ablation of pancreatic cystic lesions: the use of multiple endoscopic ultrasound-guided ethanol lavage sessions. Pancreas. 2011; 40:664–668.12. Caillol F, Poincloux L, Bories E, et al. Ethanol lavage of 14 mucinous cysts of the pancreas: a retrospective study in two tertiary centers. Endosc Ultrasound. 2012; 1:48–52.
Article13. DeWitt JM, Al-Haddad M, Sherman S, et al. Alterations in cyst fluid genetics following endoscopic ultrasound-guided pancreatic cyst ablation with ethanol and paclitaxel. Endoscopy. 2014; 46:457–464.
Article14. Gómez V, Takahashi N, Levy MJ, et al. EUS-guided ethanol lavage does not reliably ablate pancreatic cystic neoplasms (with video). Gastrointest Endosc. 2016; 83:914–920.
Article15. Choi JH, Seo DW, Song TJ, et al. Long-term outcomes after endoscopic ultrasound-guided ablation of pancreatic cysts. Endoscopy. 2017; 49:866–873.
Article16. Moyer MT, Sharzehi S, Mathew A, et al. The safety and efficacy of an alcohol-free pancreatic cyst ablation protocol. Gastroenterology. 2017; 153:1295–1303.
Article17. Choi JH, Lee SH, Choi YH, et al. Clinical outcomes of endoscopic ultrasound-guided ethanol ablation for pancreatic cystic lesions compared with the natural course: a propensity score matching analysis. Therap Adv Gastroenterol. 2018; 11:1756284818759929.
Article18. Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010; 71:446–454.
Article19. Choi JH, Lee SH, You MS, et al. Safety and adverse events of EUS-guided ethanol ablation for pancreatic cystic lesions: a single center experience. In : Joint Meeting of the Asian-Oceanic Pancreatic Association, the Korean Pancreatobiliary Association, and the Korean Pancreas Surgery Club 2018; 2018 Apr 26-28; Seoul, Korea. Seoul: Korean Pancreatobiliary Association, Korean Pancreas Surgery Club;2018. p. 386–387.20. Oh HC, Brugge WR. EUS-guided pancreatic cyst ablation: a critical review (with video). Gastrointest Endosc. 2013; 77:526–533.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Ultrasound-Guided Treatment of Pancreatic Cystic and Solid Masses
- Endoscopic ultrasound-guided ablation of pancreatic cystic lesions
- Recent developments in endoscopic ultrasound-guided ablation treatment
- Successful Endoscopic Ultrasound-Guided Alcohol Ablation of Sporadic Insulinoma Using Three-Dimensional Targeting (with Video)
- Recent developments in endoscopic ultrasound-guided diagnosis and therapy of pancreatic cystic neoplasms
