J Gastric Cancer.
2019 Mar;19(1):111-120. 10.5230/jgc.2019.19.e10.
Short-Term Outcomes of Intracorporeal Delta-Shaped Gastroduodenostomy Versus Extracorporeal Gastroduodenostomy after Laparoscopic Distal Gastrectomy for Gastric Cancer
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jar319.an@samsung.com
- 2Department of Surgery, Korea University College of Medicine, Seoul, Korea.
- 3Department of Surgery, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2458823
- DOI: http://doi.org/10.5230/jgc.2019.19.e10
Abstract
- BACKGROUND
Billroth I anastomosis is one of the most common reconstruction methods after distal gastrectomy for gastric cancer. Intracorporeal Billroth I (ICBI) anastomosis and extracorporeal Billroth I (ECBI) anastomosis are widely used in laparoscopic surgery. Here we compared ICBI and ECBI outcomes at a major gastric cancer center.
METHODS
We retrospectively analyzed data from 2,284 gastric cancer patients who underwent laparoscopic distal gastrectomy between 2009 and 2017. We divided the subjects into ECBI (n=1,681) and ICBI (n=603) groups, compared the patients' clinical characteristics and surgical and short-term outcomes, and performed risk factor analyses of postoperative complication development.
RESULTS
The ICBI group experienced shorter operation times, less blood loss, and shorter hospital stays than the ECBI group. There were no clinically significant intergroup differences in diet initiation. Changes in white blood cell counts and C-reactive protein levels were similar between groups. Grade II-IV surgical complication rates were 2.7% and 4.0% in the ECBI and ICBI groups, respectively, with no significant intergroup differences. Male sex and a body mass index (BMI) ≥30 were independent risk factors for surgical complication development. In the ECBI group, patients with a BMI ≥30 experienced a significantly higher surgical complication rate than those with a lower BMI, while no such difference was observed in the ICBI group.
CONCLUSION
The surgical safety of ICBI was similar to that of ECBI. Although the chosen anastomotic technique was not a risk factor for surgical complications, ECBI was more vulnerable to surgical complications than ICBI in patients with a high BMI (≥30).
Keyword
MeSH Terms
Figure
-
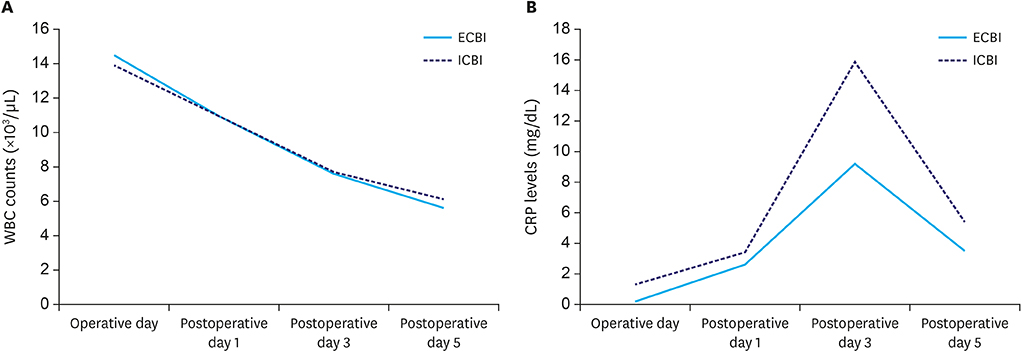
Fig. 1 Postoperative inflammatory response in the ECBI and ICBI groups. (A) WBC counts of each reconstruction method after laparoscopic gastrectomy. (B) CRP levels by reconstruction method after laparoscopic gastrectomy. ECBI, = extracorporeal Billroth I; ICBI, = intracorporeal Billroth I; WBC = white blood cell; CRP = C-reactive protein.
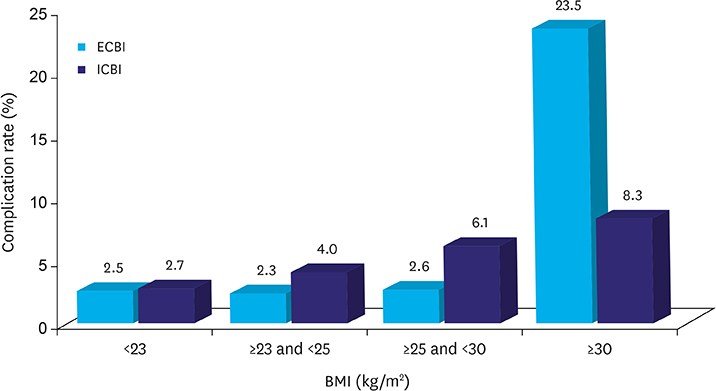
Fig. 2 Complication rate according to BMI changes in the ECBI and ICBI groups. BMI = body mass index; ECBI = extracorporeal Billroth I; ICBI = intracorporeal Billroth I.
Reference
-
1. Yang HK. Current status of clinical practice for gastric cancer patients in Korea: a nationwide survey. J Korean Gastric Cancer Assoc. 2004; 4:95–108.
Article2. Kim BJ, O'Connell T. Gastroduodenostomy after gastric resection for cancer. Am Surg. 1999; 65:905–907.3. Kumagai K, Shimizu K, Yokoyama N, Aida S, Arima S, Aikou T, et al. Questionnaire survey regarding the current status and controversial issues concerning reconstruction after gastrectomy in Japan. Surg Today. 2012; 42:411–418.
Article4. Lee JH, Hyung WJ, Kim HI, Kim YM, Son T, Okumura N, et al. Method of reconstruction governs iron metabolism after gastrectomy for patients with gastric cancer. Ann Surg. 2013; 258:964–969.
Article5. Song KY, Park CH, Kang HC, Kim JJ, Park SM, Jun KH, et al. Is totally laparoscopic gastrectomy less invasive than laparoscopy-assisted gastrectomy?: prospective, multicenter study. J Gastrointest Surg. 2008; 12:1015–1021.
Article6. Kinoshita T, Shibasaki H, Oshiro T, Ooshiro M, Okazumi S, Katoh R. Comparison of laparoscopy-assisted and total laparoscopic Billroth-I gastrectomy for gastric cancer: a report of short-term outcomes. Surg Endosc. 2011; 25:1395–1401.
Article7. Kim BS, Yook JH, Choi YB, Kim KC, Kim MG, Kim TH, et al. Comparison of early outcomes of intracorporeal and extracorporeal gastroduodenostomy after laparoscopic distal gastrectomy for gastric cancer. J Laparoendosc Adv Surg Tech A. 2011; 21:387–391.
Article8. Okabe H, Obama K, Tsunoda S, Tanaka E, Sakai Y. Advantage of completely laparoscopic gastrectomy with linear stapled reconstruction: a long-term follow-up study. Ann Surg. 2014; 259:109–116.9. Ding W, Tan Y, Xue W, Wang Y, Xu XZ. Comparison of the short-term outcomes between delta-shaped anastomosis and conventional Billroth I anastomosis after laparoscopic distal gastrectomy: a meta-analysis. Medicine (Baltimore). 2018; 97:e0063.10. Wang SY, Hong J, Hao HK. A comparative study of delta-shaped and conventional Billroth I anastomosis after laparoscopic distal gastrectomy for gastric cancer. Surg Endosc. 2017; 31:3191–3202.
Article11. Tanimura S, Higashino M, Fukunaga Y, Takemura M, Nishikawa T, Tanaka Y, et al. Intracorporeal Billroth 1 reconstruction by triangulating stapling technique after laparoscopic distal gastrectomy for gastric cancer. Surg Laparosc Endosc Percutan Tech. 2008; 18:54–58.
Article12. Kanaya S, Gomi T, Momoi H, Tamaki N, Isobe H, Katayama T, et al. Delta-shaped anastomosis in totally laparoscopic Billroth I gastrectomy: new technique of intraabdominal gastroduodenostomy. J Am Coll Surg. 2002; 195:284–287.13. Kim DG, Choi YY, An JY, Kwon IG, Cho I, Kim YM, et al. Comparing the short-term outcomes of totally intracorporeal gastroduodenostomy with extracorporeal gastroduodenostomy after laparoscopic distal gastrectomy for gastric cancer: a single surgeon’s experience and a rapid systematic review with meta-analysis. Surg Endosc. 2013; 27:3153–3161.
Article14. Sobin LH, Gospodarowicz MK, Wittekind C. TNM Classification of Malignant Tumors. 7th ed. New York (NY): Wiley-Blackwell;2011.15. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009; 250:187–196.16. Kim JJ, Song KY, Chin HM, Kim W, Jeon HM, Park CH, et al. Totally laparoscopic gastrectomy with various types of intracorporeal anastomosis using laparoscopic linear staplers: preliminary experience. Surg Endosc. 2008; 22:436–442.
Article17. Ikeda T, Kawano H, Hisamatsu Y, Ando K, Saeki H, Oki E, et al. Progression from laparoscopic-assisted to totally laparoscopic distal gastrectomy: comparison of circular stapler (i-DST) and linear stapler (BBT) for intracorporeal anastomosis. Surg Endosc. 2013; 27:325–332.
Article18. Kim MG, Kawada H, Kim BS, Kim TH, Kim KC, Yook JH, et al. A totally laparoscopic distal gastrectomy with gastroduodenostomy (TLDG) for improvement of the early surgical outcomes in high BMI patients. Surg Endosc. 2011; 25:1076–1082.
Article19. Byun C, Cui LH, Son SY, Hur H, Cho YK, Han SU. Linear-shaped gastroduodenostomy (LSGD): safe and feasible technique of intracorporeal Billroth I anastomosis. Surg Endosc. 2016; 30:4505–4514.
Article20. Lee HH, Song KY, Lee JS, Park SM, Kim JJ. Delta-shaped anastomosis, a good substitute for conventional Billroth I technique with comparable long-term functional outcome in totally laparoscopic distal gastrectomy. Surg Endosc. 2015; 29:2545–2552.
Article21. Jeong O, Jung MR, Park YK, Ryu SY. Safety and feasibility during the initial learning process of intracorporeal Billroth I (delta-shaped) anastomosis for laparoscopic distal gastrectomy. Surg Endosc. 2015; 29:1522–1529.
Article22. Lin M, Zheng CH, Huang CM, Li P, Xie JW, Wang JB, et al. Totally laparoscopic versus laparoscopy-assisted Billroth-I anastomosis for gastric cancer: a case-control and case-matched study. Surg Endosc. 2016; 30:5245–5254.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intracorporeal modified delta-shaped gastroduodenostomy during 2-port distal gastrectomy: technical aspects and short-term outcomes
- Linear-Shaped Gastroduodenostomy in Totally Laparoscopic Distal Gastrectomy
- The Early Experience with a Totally Laparoscopic Distal Gastrectomy
- Long-term Functional and Patientreported Outcomes Between Intra-corporeal Delta-shaped Gastroduodenostomy and Gastrojejunostomy After Laparoscopic Distal Gastrectomy
- Intracorporeal Anastomosis Using Linear Stapler in Laparoscopic Distal Gastrectomy: Comparison between Gastroduodenostomy and Gastrojejunostomy
