A Rare Case of Adenosquamous Carcinoma Arising in the Background of IgG4-Related Lung Disease
- Affiliations
-
- 1Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hanjho@skku.edu
- 2Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2449342
- DOI: http://doi.org/10.4132/jptm.2019.02.21
Abstract
- IgG4-related disease is a systemic inflammatory disease and is known as IgG4-related lung disease (IgG4-RLD) when it involves the respiratory system. Primary lung cancer arising from a background of IgG4-RLD is very rare. Herein, we report a case of adenosquamous carcinoma arising from the background of IgG4-RLD and presenting as an interstitial lung disease pattern. A 66-year-old man underwent lobectomy under the impression of primary lung cancer. Grossly, the mass was ill-defined and gray-tan colored, and the background lung was fibrotic. Microscopically, tumor cells showed both squamous and glandular differentiation. Dense lymphoplasmacytic infiltration with fibrosis and obliterative phlebitis were seen in the background lung. IgG4 immunohistochemical stain showed diffuse positivity in infiltrating plasma cells. Primary lung adenosquamous carcinoma has not been reported in a background of IgG4-RLD. Due to the rarity of IgG4-RLD, physicians must follow patients with IgG4-RLD over long periods of time to accurately predict the risk of lung cancer.
Keyword
MeSH Terms
Figure
-
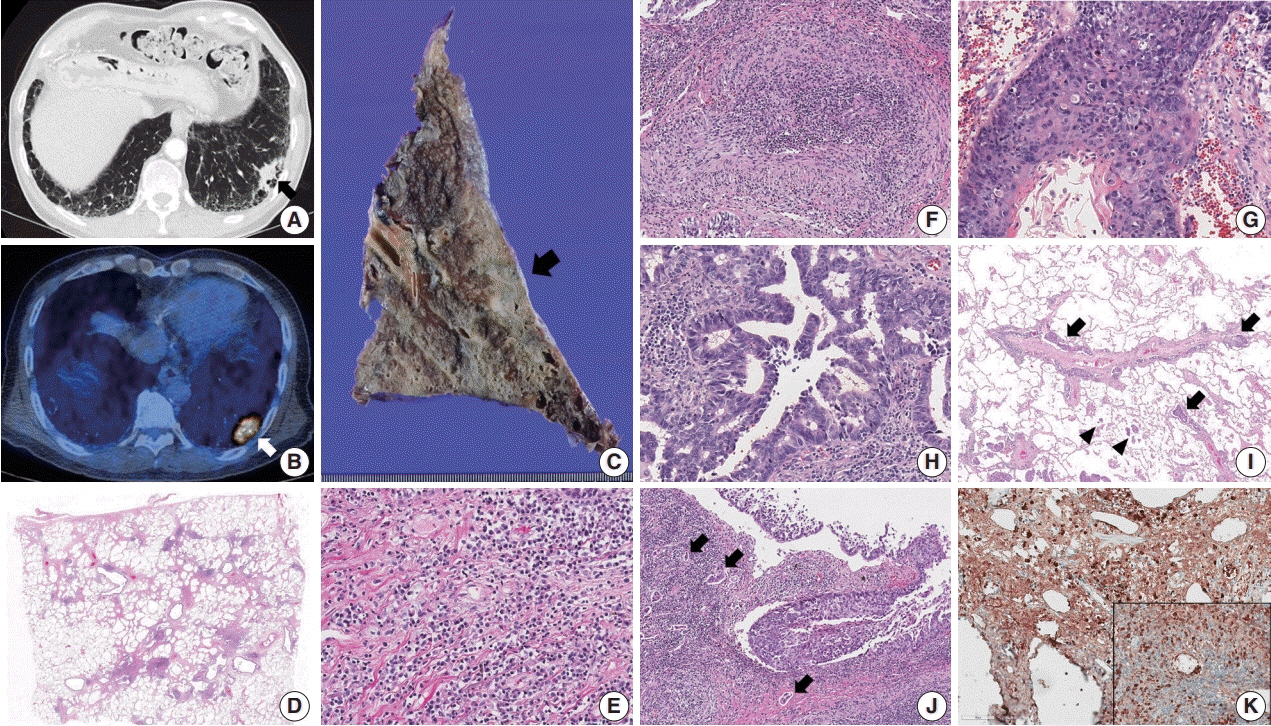
Fig. 1. (A, B) Chest computed tomography shows a consolidative nodule (arrow) in a background of subpleural reticulation and honeycomb fibrosis at both lung bases. Positron emission tomography reveals 18F-fluorodeoxyglucose uptake by the nodule. (C) The cut section of the lung showed an ill-defined and gray-tan colored mass (arrow). The background lung was emphysematous and fibrotic. (D–F) Histologic examination shows irregular interstitial fibrosis with patchy lymphoid aggregation, predominant lymphoplasmacytic infiltration, and occasional obliterative phlebitis. (G) The squamous cell carcinoma component shows keratinization and multifocal dyskeratosis. (H) The adenocarcinoma component was mainly composed of a moderately differentiated acinar pattern. (I) Diffuse spread through air space (arrowheads) and multifocal lymphangitic spread (arrow) of tumor cells are frequently found at the periphery of the mass. (J) Dense fibrosis and lymphoplasmacytic infiltration are found in the peritumoral area. Multifocal endolymphatic tumor emboli (arrows) are also noted. (K) Both IgG4 and IgG (inset) immunohistochemical stains show diffuse positivity in the infiltrating plasma cells. The IgG4/IgG ratio was over 40%.
Reference
-
1. Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012; 25:1181–92.2. Ahn JH, Hong SI, Cho DH, Chae EJ, Song JS, Song JW. A case of IgG4-related lung disease presenting as interstitial lung disease. Tuberc Respir Dis. 2014; 77:85–9.
Article3. Cho DH, An JH, Kang YM, Chae EJ, Song JS, Song JW. A case of IgG4-related lung disease mimicking non-specific interstitial pneumonia. Korean J Med. 2015; 88:308–12.
Article4. Zen Y, Inoue D, Kitao A, et al. IgG4-related lung and pleural disease: a clinicopathologic study of 21 cases. Am J Surg Pathol. 2009; 33:1886–93.
Article5. Inoue T, Hayama M, Kobayashi S, et al. Lung cancer complicated with IgG4-related disease of the lung. Ann Thorac Cardiovasc Surg. 2014; 20 Suppl:474–7.
Article6. Tashiro H, Takahashi K, Nakamura T, Komiya K, Kimura S, Sueoka-Aragane N. Coexistence of lung cancer and immunoglobulin G4-related lung disease in a nodule: a case report. J Med Case Rep. 2016; 10:113.
Article7. Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001; 344:732–8.
Article8. Fei Y, Shi J, Lin W, et al. Intrathoracic involvements of immunoglobulin G4-related sclerosing disease. Medicine (Baltimore). 2015; 94:e2150.
Article9. Yamamoto M, Takahashi H, Tabeya T, et al. Risk of malignancies in IgG4-related disease. Mod Rheumatol. 2012; 22:414–8.
Article10. Hirano K, Tada M, Sasahira N, et al. Incidence of malignancies in patients with IgG4-related disease. Intern Med. 2014; 53:171–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Adenosquamous Carcinoma Arising from the Tonsil
- Immunoglobulin G4-Related Lung Disease Mimicking Lung Cancer: Two Case Reports
- A Case of Adenosquamous Carcinoma Ex Pleomorphic Adenoma of Submandibular Gland
- A Case of Cutaneous Metastatic Adenosquamous Carcinoma of the Pancreas
- Metastatic Cutaneous Adenosquamous Carcinoma in a Patient Undergoing Chemotherapy for Lung Adenocarcinoma
