Short-term Efficacy and Safety of Ranibizumab for Neovascular Age-related Macular Degeneration in the Real World: A Post-marketing Surveillance Study
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Korea. sejoon1@snu.ac.kr
- 2Novartis Korea, Seoul, Korea.
- 3Hyemin Eye Hospital, Seoul, Korea.
- KMID: 2442620
- DOI: http://doi.org/10.3341/kjo.2018.0081
Abstract
- PURPOSE
To investigate the short-term efficacy and safety of ranibizumab in the routine clinical setting in patients with neovascular age-related macular degeneration and to analyze the associated factors for visual outcome.
METHODS
This was a post-hoc analysis of a ranibizumab regulatory post-marketing surveillance study in which 4,136 patients were enrolled and followed for 12 weeks. Change in best-corrected visual acuity (BCVA), size of choroidal neovascularization, and the presence of hemorrhage and exudate were analyzed and the association between BCVA change and baseline characteristics were investigated. Data on ocular and systemic adverse events were collected.
RESULTS
Mean BCVA improved significantly and mean BCVA change was the logarithm of the minimal angle of resolution 0.13 ± 0.01 (p < 0.001). A lower baseline BCVA and younger age were significant predictive factors for visual improvement or maintenance (≥0 lines). For greater visual acuity gain (≥3 lines), no treatment history, lower baseline BCVA, younger age, and classic-type choroidal neovascularization were significant predictive factors. No new safety signals were found.
CONCLUSIONS
In this study, conducted in real-world clinical practice with a large number of neovascular age-related macular degeneration patients, visual and anatomical outcomes improved significantly after three monthly ranibizumab treatments. Treatment-naive patients had a higher chance of greater visual gain (≥3 lines) than non-naive patients.
Keyword
MeSH Terms
Figure
-
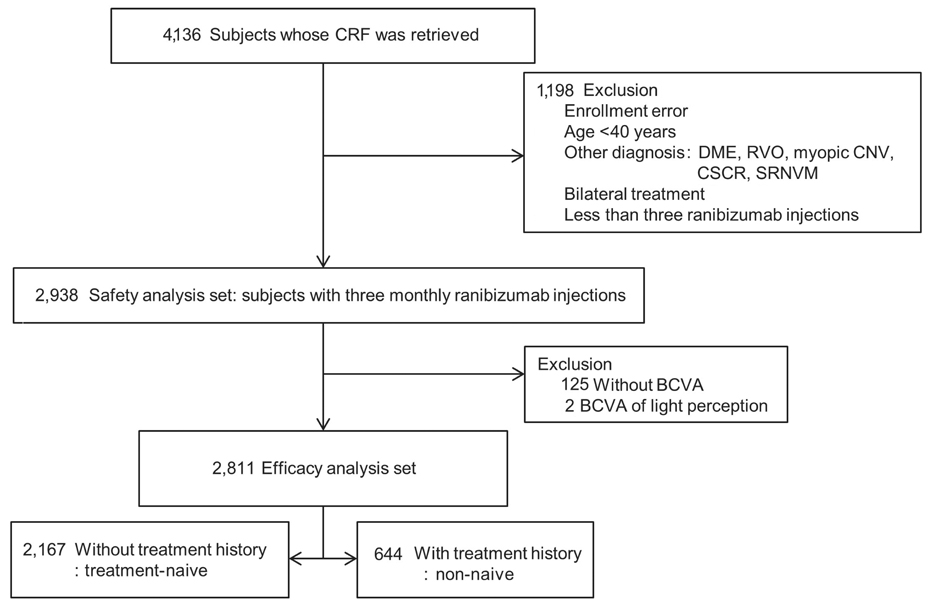
Fig. 1 Flow charts of grouping subjects enrolled in the ranibizumab regulatory post-marketing surveillance study. CRF = case report form; DME = diabetic macular edema; RVO = retinal vein occlusion; CNV = choroidal neovascularization; CSCR = central serous chorioretinopathy; SRNVM = subretinal neovascular membrane; BCVA = best-corrected visual acuity.
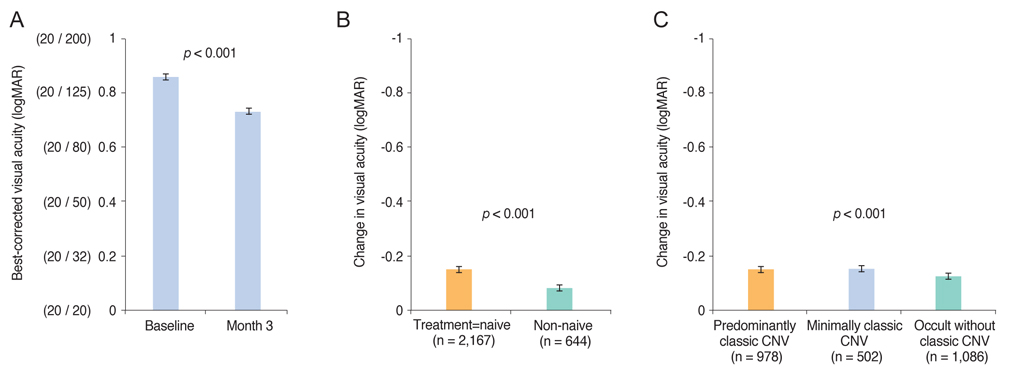
Fig. 2 Changes of best-corrected visual acuity after three monthly ranibizumab injections. (A) Best-corrected visual acuity (BCVA, mean ± standard deviation) of 2,811 subjects in the efficacy analysis set improved at three months from baseline (Wilcoxon signed rank test, p < 0.001). (B) Eyes of treatment-naive group achieved greater BCVA (mean ± standard error) gain compared to those of non-naive group (Wilcoxon rank sum test, p < 0.001). (C) Changes of BCVA were different among the three different choroidal neovascularization (CNV) groups (Kruskal-Wallis test, p < 0.001). logMAR = logarithm of minimum angle resolution.
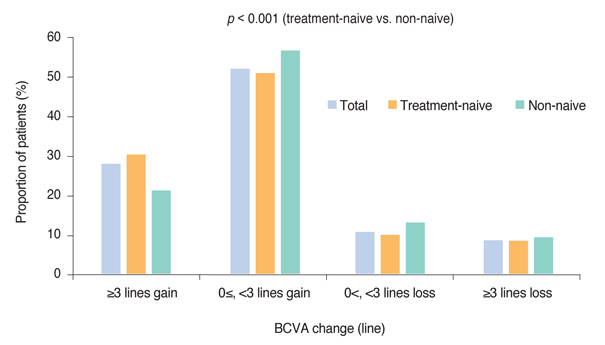
Fig. 3 Proportion of patients with visual change categorized as logarithm of the minimum angle of resolution ≤−0.3 (Early Treatment Diabetic Retinopathy Study 3 or more lines gain); 0 to −0.3 (<3 lines gain or no change); 0.3 to 0 (<3 lines loss); and 0.3 (3 or more lines loss) in total, treatment-naive, and non-naive groups. The distribution of visual gain or loss was statistically different between the naive and non-naive groups (chi-square test, p < 0.001). BCVA = best-corrected visual acuity.
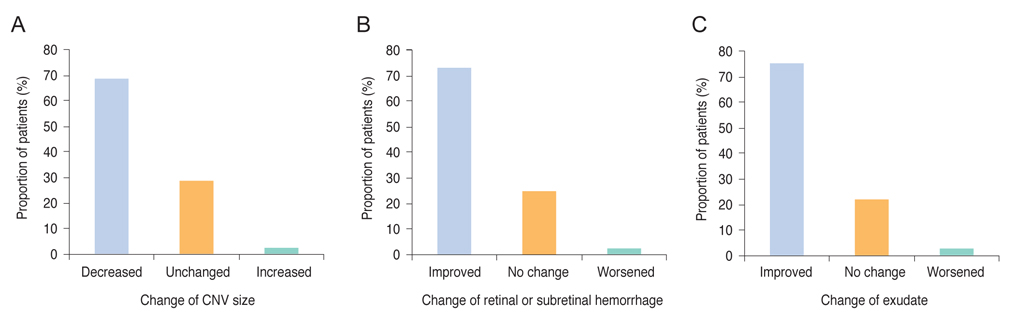
Fig. 4 Anatomical changes including choroidal neovascularization (CNV) size (A), retinal or subretinal hemorrhage (B), and exudate (C) after three monthly injections of ranibizumab on the total patients (n = 2,811) in the efficacy analysis set.
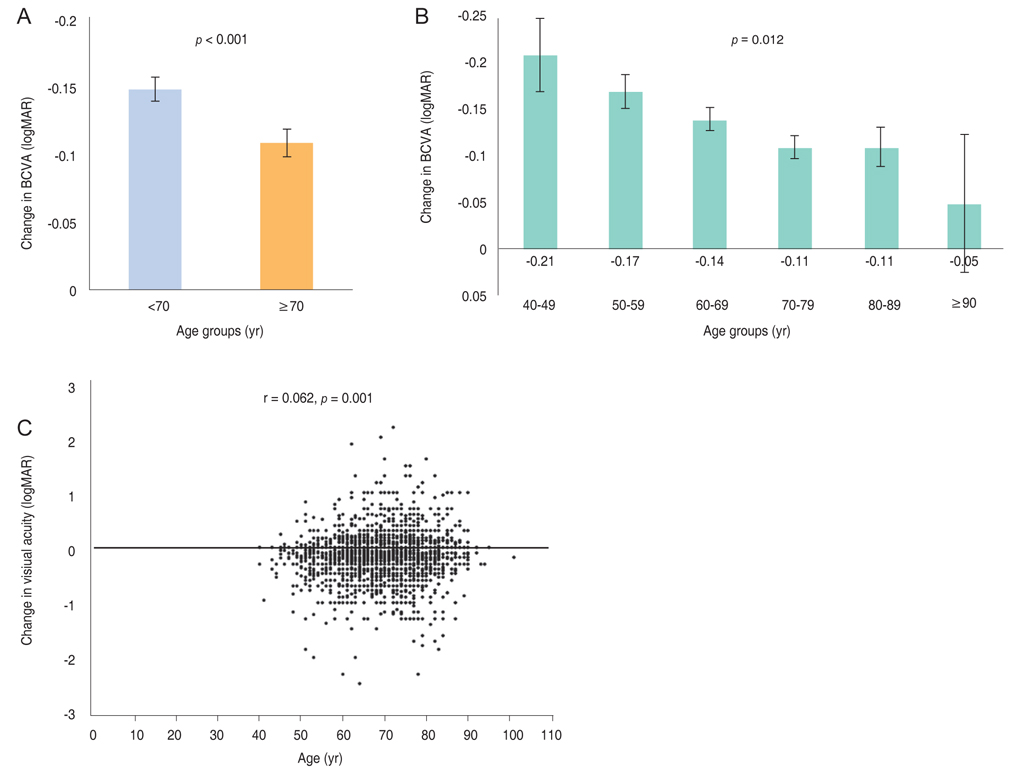
Fig. 5 Comparison of best-corrected visual acuity (BCVA) changes according to the age groups. (A) BCVA (mean ± standard error) improved in both <70 and ≥70 years age groups significantly from baseline (Wilcoxon signed rank test, both p < 0.001), however, the change is greater in the younger age group (Wilcoxon rank sum test, p < 0.001). (B) BCVA improved in all age groups (Wilcoxon signed rank test, p < 0.05) except for the oldest age group (p = 0.074) and the change in BCVA was different among the six age groups (Kruskal-Wallis test, p < 0.001). (C) BCVA change was correlated with age (r = 0.062, p = 0.001). logMAR = logarithm of minimum angle resolution.

Fig. 6 Comparison of best-correct visual acuity (BCVA) changes according to the baseline visual acuity. (A) BCVA (mean ± standard error) improved in both <20 / 100 and ≥20 / 100 groups significantly from baseline (Wilcoxon signed rank test, both p < 0.001) and the change was greater in the worse baseline visual acuity group (Wilcoxon rank sum test, p < 0.001). (B,C) BCVA improved in three baseline BCVA groups (Wilcoxon signed rank test, p < 0.05) but not for the group with the best baseline BCVA ( p = 0.351). The changes in BCVA were different among the four baseline BCVA groups (Kruskal-Wallis test, p < 0.001) and correlated with baseline BCVA (r = 0.331, p < 0.001). logMAR = logarithm of minimum angle resolution.

Fig. 7 Graphs showing baseline predictive factors associated with (A,B) a visual gain or no change from baseline best-corrected visual acuity (BCVA) and those associated with (C,D) a gain of 3 or more lines from baseline BCVA. (A) Age less than 70 years and baseline BCVA worse than 20 / 100 were the significant predictors for BCVA gain or no change (p = 0.083 and p < 0.001, respectively) in model 1. (B) In model 2, age group 40 to 49 years (p = 0.049) and baseline BCVA group <20 / 320, 20 / 320 to 20 / 100, 20 / 100 to 20 / 40 were the significant predictors for BCVA gain or no change. (C) No treatment history (p < 0.001), age less than 70 years (p < 0.001), baseline BCVA worse than 20 / 100 (p < 0.001), choroidal neovascularization (CNV) with predominantly classic CNV (p = 0.002), and minimally classic CNV (p = 0.017) were associated with BCVA gain of 3 or more lines. (D) In model 2, no prior treatment history (p < 0.001), age of 40 to 49 years (p = 0.004), baseline BCVA of <20 / 320, 20 / 320 to 20 / 100, 20 / 100 to 20 / 40 (all p < 0.001), predominantly classic CNV (p = 0.005), and minimally classic CNV (p = 0.024) were the significant predictors for BCVA gain of three or more lines. *Versus occult without classic CNV.
Reference
-
1. Bressler NM. Age-related macular degeneration is the leading cause of blindness. JAMA. 2004; 291:1900–1901.2. Lee PP, Feldman ZW, Ostermann J, et al. Longitudinal prevalence of major eye diseases. Arch Ophthalmol. 2003; 121:1303–1310.
Article3. Park SJ, Lee JH, Woo SJ, et al. Age-related macular degeneration: prevalence and risk factors from Korean National Health and Nutrition Examination Survey, 2008 through 2011. Ophthalmology. 2014; 121:1756–1765.4. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006; 355:1419–1431.
Article5. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006; 355:1432–1444.
Article6. Kim JH, Lee DW, Chang YS, et al. Twelve-month outcomes of treatment using ranibizumab or aflibercept for neovascular age-related macular degeneration: a comparative study. Graefes Arch Clin Exp Ophthalmol. 2016; 254:2101–2109.
Article7. Kang HM, Koh HJ. Long-term visual outcome and prognostic factors after intravitreal ranibizumab injections for polypoidal choroidal vasculopathy. Am J Ophthalmol. 2013; 156:652–660.
Article8. Shin JY, Yu HG. Optical coherence tomography-based ranibizumab monotherapy for retinal angiomatous proliferation in Korean patients. Retina. 2014; 34:2359–2366.
Article9. Ogura Y, Terasaki H, Gomi F, et al. Efficacy and safety of intravitreal aflibercept injection in wet age-related macular degeneration: outcomes in the Japanese subgroup of the VIEW 2 study. Br J Ophthalmol. 2015; 99:92–97.
Article10. Lee FL, Kwon OW, Chung H, et al. Ranibizumab in South Korean and Taiwanese patients with age-related macular degeneration: primary outcome of the EXTEND III study. Acta Ophthalmol. 2012; 90:e406–e407.
Article11. Holladay JT. Proper method for calculating average visual acuity. J Refract Surg. 1997; 13:388–391.
Article12. CATT Research Group. Martin DF, Maguire MG, et al. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011; 364:1897–1908.
Article13. Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012; 119:2537–2548.
Article14. Ying GS, Huang J, Maguire MG, et al. Baseline predictors for one-year visual outcomes with ranibizumab or bevacizumab for neovascular age-related macular degeneration. Ophthalmology. 2013; 120:122–129.
Article15. Ying GS, Maguire MG, Daniel E, et al. Association of baseline characteristics and early vision response with 2-year vision outcomes in the Comparison of AMD Treatments Trials (CATT). Ophthalmology. 2015; 122:2523–2531.
Article16. Grunwald JE, Daniel E, Huang J, et al. Risk of geographic atrophy in the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2014; 121:150–161.17. Grunwald JE, Pistilli M, Daniel E, et al. Incidence and growth of geographic atrophy during 5 years of comparison of age-related macular degeneration treatments trials. Ophthalmology. 2017; 124:97–104.
Article18. Grunwald JE, Pistilli M, Ying GS, et al. Growth of geographic atrophy in the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2015; 122:809–816.
Article19. Boyer DS, Antoszyk AN, Awh CC, et al. Subgroup analysis of the MARINA study of ranibizumab in neovascular age-related macular degeneration. Ophthalmology. 2007; 114:246–252.
Article20. Kaiser PK, Brown DM, Zhang K, et al. Ranibizumab for predominantly classic neovascular age-related macular degeneration: subgroup analysis of first-year ANCHOR results. Am J Ophthalmol. 2007; 144:850–857.
Article21. Rosenfeld PJ, Shapiro H, Tuomi L, et al. Characteristics of patients losing vision after 2 years of monthly dosing in the phase III ranibizumab clinical trials. Ophthalmology. 2011; 118:523–530.
Article22. Chen M, Rajapakse D, Fraczek M, et al. Retinal pigment epithelial cell multinucleation in the aging eye: a mechanism to repair damage and maintain homoeostasis. Aging Cell. 2016; 15:436–445.23. Park SJ, Kwon KE, Choi NK, et al. Prevalence and incidence of exudative age-related macular degeneration in South Korea: a nationwide population-based study. Ophthalmology. 2015; 122:2063–2070.24. Holz FG, Bandello F, Gillies M, et al. Safety of ranibizumab in routine clinical practice: 1-year retrospective pooled analysis of four European neovascular AMD registries within the LUMINOUS programme. Br J Ophthalmol. 2013; 97:1161–1167.
Article25. Wolf A, Kampik A. Efficacy of treatment with ranibizumab in patients with wet age-related macular degeneration in routine clinical care: data from the COMPASS health services research. Graefes Arch Clin Exp Ophthalmol. 2014; 252:647–655.
Article26. Cohen SY, Mimoun G, Oubraham H, et al. Changes in visual acuity in patients with wet age-related macular degeneration treated with intravitreal ranibizumab in daily clinical practice: the LUMIERE study. Retina. 2013; 33:474–481.27. Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group. Martin DF, Maguire MG, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012; 119:1388–1398.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Five-year Outcomes of Ranibizumab in Neovascular Age-related Macular Degeneration: Real Life Clinical Experience
- Efficacy of Three Aflibercept Injections for Neovascular Age-related Macular Degeneration Showing Limited Response to Ranibizumab
- Intravitreal Ranibizumab Therapy for Neovascular Age-Related Macular Degeneration with a Predominantly Hemorrhagic Lesion
- Intravitreal Aflibercept for Neovascular Age-Related Macular Degeneration Resistant to Bevacizumab and Ranibizumab
- Safety and efficacy of fimasartan with essential hypertension patients in real world clinical practice: data from a post marketing surveillance in Korea
