How do we manage high-grade T1 bladder cancer? Conservative or aggressive therapy?
- Affiliations
-
- 1Department of Urology, Chungbuk National University College of Medicine, Cheongju, Korea. sjyun@chungbuk.ac.kr
- 2Medical Genomics Research Center, Research Institute of Bioscience and Biotechnology, Daejeon, Korea.
- 3Korean Bioinformation Center, Research Institute of Bioscience and Biotechnology, Daejeon, Korea.
- KMID: 2426516
- DOI: http://doi.org/10.4111/icu.2016.57.S1.S44
Abstract
- High-grade T1 bladder cancer has a poor prognosis due to a higher incidence of recurrence and progression than other nonmuscle invasive bladder cancer; thus patients with high-grade T1 have to be carefully monitored and managed. If patients are diagnosed with high-grade T1 at initial transurethral resection (TUR), a second TUR is strongly recommended regardless of whether muscle layer is present in the specimen because of the possibility of understating due to incomplete resection. Since high-grade T1 disease shows diverse clinical courses, individual approaches are recommended for treatment. In cases with low risk of progression, cystectomy could represent overtreatment and deteriorate quality of life irreversibly, while, in those with high risk, bacillus Calmette-Guérin (BCG) therapy may worsen survival by delaying definitive therapy. Therefore, a strategy for predicting prognosis based on the risk of progression is needed for managing high-grade T1 disease. Molecular risk classifiers predicting the risk of progression and response to BCG may help identify the optimal management of high-grade T1 disease for each individual.
MeSH Terms
Figure
-

Fig. 1 T1 disease substaging systems based on depth or width of tumor infiltration. T1a, invasion above muscularis mucosae; T1b, invasion within muscularis mucosae; T1c, invasion below muscularis mucosae; T1m, a single focus of lamina propria invasion ≤0.5 mm; T1e, specimens showing >0.5 mm lamina propria invasion or multiple invasions.
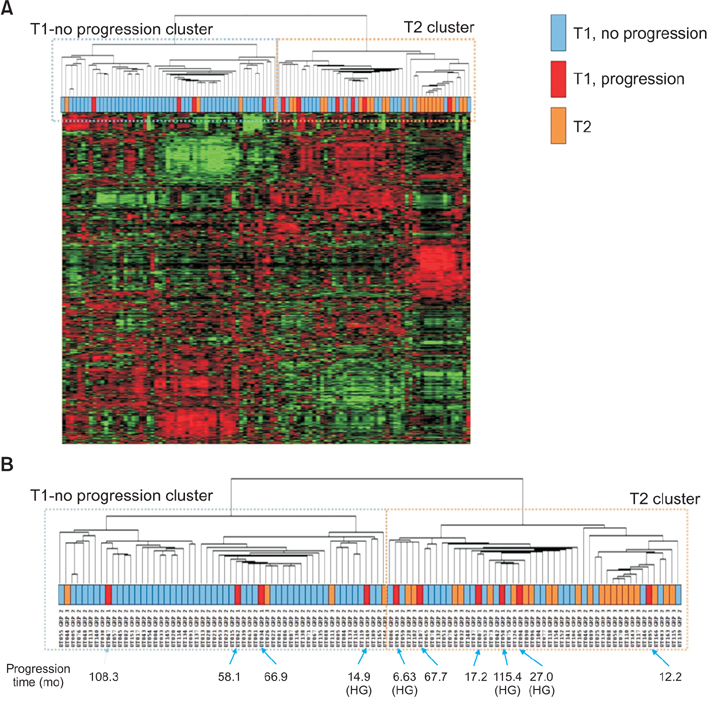
Fig. 2 Unsupervised hierarchical clustering using 70 patients with T1 who did not experience progression, 10 patients with T1 who experienced progression, and 26 patients with T2 disease (GSE 13507). Interestingly, three of four patients with high-grade T1 who experienced progression were categorized as T2. This means that high-grade T1 gene expression patterns might already have muscle invasive bladder cancer characteristics at initial diagnosis. (A) Heatmap from microarray data. (B) Clustering with clinico-pathological variables. HG, high-grade.
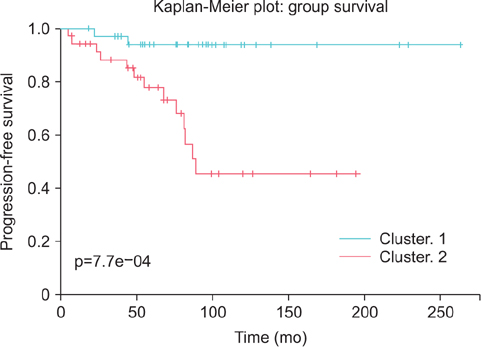
Fig. 3 Long-term validation study of the progression-related gene classifier in patients with nonmuscle invasive bladder cancer. Progression-related eight-gene classifier could accurately predict the progression of nonmuscle invasive bladder cancer.

Fig. 4 Proposed algorithm for decision-making in high-grade T1 bladder cancer. TUR, transurethral resection; CIS, carcinoma in situ; BCG, bacillus Calmette-Guérin.
Reference
-
1. Oh CM, Won YJ, Jung KW, Kong HJ, Cho H, Lee JK, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2013. Cancer Res Treat. 2016; 48:436–450.2. Song W, Jeon HG. Incidence of kidney, bladder, and prostate cancers in Korea: An update. Korean J Urol. 2015; 56:422–428.3. Sylvester RJ, van der Meijden AP, Oosterlinck W, Witjes JA, Bouffioux C, Denis L, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006; 49:466–477.4. Sylvester RJ, van der Meijden AP, Lamm DL. Intravesical bacillus Calmette-Guerin reduces the risk of progression in patients with superficial bladder cancer: a meta-analysis of the published results of randomized clinical trials. J Urol. 2002; 168:1964–1970.5. Malmström PU, Sylvester RJ, Crawford DE, Friedrich M, Krege S, Rintala E, et al. An individual patient data meta-analysis of the long-term outcome of randomised studies comparing intravesical mitomycin C versus bacillus Calmette-Guérin for non-muscle-invasive bladder cancer. Eur Urol. 2009; 56:247–256.6. Kulkarni GS, Hakenberg OW, Gschwend JE, Thalmann G, Kassouf W, Kamat A, et al. An updated critical analysis of the treatment strategy for newly diagnosed high-grade T1 (previously T1G3) bladder cancer. Eur Urol. 2010; 57:60–70.7. van den Bosch S, Alfred Witjes J. Long-term cancer-specific survival in patients with high-risk, non-muscle-invasive bladder cancer and tumour progression: a systematic review. Eur Urol. 2011; 60:493–500.8. Mariappan P, Finney SM, Head E, Somani BK, Zachou A, Smith G, et al. Good quality white-light transurethral resection of bladder tumours (GQ-WLTURBT) with experienced surgeons performing complete resections and obtaining detrusor muscle reduces early recurrence in new non-muscle-invasive bladder cancer: validation across time and place and recommendation for benchmarking. BJU Int. 2012; 109:1666–1673.9. Richterstetter M, Wullich B, Amann K, Haeberle L, Engehausen DG, Goebell PJ, et al. The value of extended transurethral resection of bladder tumour (TURBT) in the treatment of bladder cancer. BJU Int. 2012; 110(2 Pt 2):E76–E79.10. Mashni J, Godoy G, Haarer C, Dalbagni G, Reuter VE, Al-Ahmadie H, et al. Prospective evaluation of plasma kinetic bipolar resection of bladder cancer: comparison to monopolar resection and pathologic findings. Int Urol Nephrol. 2014; 46:1699–1705.11. Venkatramani V, Panda A, Manojkumar R, Kekre NS. Monopolar versus bipolar transurethral resection of bladder tumors: a single center, parallel arm, randomized, controlled trial. J Urol. 2014; 191:1703–1707.12. Schumacher MC, Holmang S, Davidsson T, Friedrich B, Pedersen J, Wiklund NP. Transurethral resection of non-muscle-invasive bladder transitional cell cancers with or without 5-aminolevulinic Acid under visible and fluorescent light: results of a prospective, randomised, multicentre study. Eur Urol. 2010; 57:293–299.13. Stenzl A, Penkoff H, Dajc-Sommerer E, Zumbraegel A, Hoeltl L, Scholz M, et al. Detection and clinical outcome of urinary bladder cancer with 5-aminolevulinic acid-induced fluorescence cystoscopy : A multicenter randomized, double-blind, placebo-controlled trial. Cancer. 2011; 117:938–947.14. Herr HW. Randomized trial of narrow-band versus white-light cystoscopy for restaging (second-look) transurethral resection of bladder tumors. Eur Urol. 2015; 67:605–608.15. Ramírez-Backhaus M, Dominguez-Escrig J, Collado A, Rubio-Briones J, Solsona E. Restaging transurethral resection of bladder tumor for high-risk stage Ta and T1 bladder cancer. Curr Urol Rep. 2012; 13:109–114.16. Shim JS, Choi H, Noh TI, Tae JH, Yoon SG, Kang SH, et al. The clinical significance of a second transurethral resection for T1 high-grade bladder cancer: Results of a prospective study. Korean J Urol. 2015; 56:429–434.17. Jahnson S, Wiklund F, Duchek M, Mestad O, Rintala E, Hellsten S, et al. Results of second-look resection after primary resection of T1 tumour of the urinary bladder. Scand J Urol Nephrol. 2005; 39:206–210.18. Vasdev N, Dominguez-Escrig J, Paez E, Johnson MI, Durkan GC, Thorpe AC. The impact of early re-resection in patients with pT1 high-grade non-muscle invasive bladder cancer. Ecancermedicalscience. 2012; 6:269.19. Miladi M, Peyromaure M, Zerbib M, Saighi D, Debre B. The value of a second transurethral resection in evaluating patients with bladder tumours. Eur Urol. 2003; 43:241–245.20. Schwaibold HE, Sivalingam S, May F, Hartung R. The value of a second transurethral resection for T1 bladder cancer. BJU Int. 2006; 97:1199–1201.21. Kim W, Song C, Park S, Kim J, Park J, Kim SC, et al. Value of immediate second resection of the tumor bed to improve the effectiveness of transurethral resection of bladder tumor. J Endourol. 2012; 26:1059–1064.22. Herr HW, Donat SM, Dalbagni G. Can restaging transurethral resection of T1 bladder cancer select patients for immediate cystectomy? J Urol. 2007; 177:75–79.23. Mungan MU, Canda AE, Tuzel E, Yorukoglu K, Kirkali Z. Risk factors for mucosal prostatic urethral involvement in superficial transitional cell carcinoma of the bladder. Eur Urol. 2005; 48:760–763.24. Platz CE, Cohen MB, Jones MP, Olson DB, Lynch CF. Is microstaging of early invasive cancer of the urinary bladder possible or useful? Mod Pathol. 1996; 9:1035–1039.25. Smits G, Schaafsma E, Kiemeney L, Caris C, Debruyne F, Witjes JA. Microstaging of pT1 transitional cell carcinoma of the bladder: identification of subgroups with distinct risks of progression. Urology. 1998; 52:1009–1013.26. van Rhijn BW, van der Kwast TH, Alkhateeb SS, Fleshner NE, van Leenders GJ, Bostrom PJ, et al. A new and highly prognostic system to discern T1 bladder cancer substage. Eur Urol. 2012; 61:378–384.27. DE Marco V, Cerruto MA, D'Elia C, Brunelli M, Otte O, Minja A, et al. Prognostic role of substaging in T1G3 transitional cell carcinoma of the urinary bladder. Mol Clin Oncol. 2014; 2:575–580.28. Denzinger S, Otto W, Fritsche HM, Roessler W, Wieland WF, Hartmann A, et al. Bladder sparing approach for initial T1G3 bladder cancer: Do multifocality, size of tumor or concomitant carcinoma in situ matter? A long-term analysis of 132 patients. Int J Urol. 2007; 14:995–999.29. Palou J, Sylvester RJ, Faba OR, Parada R, Peña JA, Algaba F, et al. Female gender and carcinoma in situ in the prostatic urethra are prognostic factors for recurrence, progression, and disease-specific mortality in T1G3 bladder cancer patients treated with bacillus Calmette-Guérin. Eur Urol. 2012; 62:118–125.30. Gontero P, Sylvester R, Pisano F, Joniau S, Vander Eeckt K, Serretta V, et al. Prognostic factors and risk groups in T1G3 non-muscle-invasive bladder cancer patients initially treated with Bacillus Calmette-Guérin: results of a retrospective multicenter study of 2451 patients. Eur Urol. 2015; 67:74–82.31. Dalbagni G, Vora K, Kaag M, Cronin A, Bochner B, Donat SM, et al. Clinical outcome in a contemporary series of restaged patients with clinical T1 bladder cancer. Eur Urol. 2009; 56:903–910.32. Kim WJ, Kim EJ, Kim SK, Kim YJ, Ha YS, Jeong P, et al. Predictive value of progression-related gene classifier in primary non-muscle invasive bladder cancer. Mol Cancer. 2010; 9:3.33. Hurst CD, Platt FM, Taylor CF, Knowles MA. Novel tumor subgroups of urothelial carcinoma of the bladder defined by integrated genomic analysis. Clin Cancer Res. 2012; 18:5865–5877.34. Dyrskjot L, Zieger K, Real FX, Malats N, Carrato A, Hurst C, et al. Gene expression signatures predict outcome in non-muscleinvasive bladder carcinoma: a multicenter validation study. Clin Cancer Res. 2007; 13:3545–3551.35. Bartsch G Jr, Mitra AP, Mitra SA, Almal AA, Steven KE, Skinner DG, et al. Use of artificial intelligence and machine learning algorithms with gene expression profiling to predict recurrent nonmuscle invasive urothelial carcinoma of the bladder. J Urol. 2016; 195:493–498.36. Shelley MD, Wilt TJ, Court J, Coles B, Kynaston H, Mason MD. Intravesical bacillus Calmette-Guérin is superior to mitomycin C in reducing tumour recurrence in high-risk superficial bladder cancer: a meta-analysis of randomized trials. BJU Int. 2004; 93:485–490.37. Böhle A, Bock PR. Intravesical bacille Calmette-Guérin versus mitomycin C in superficial bladder cancer: formal meta-analysis of comparative studies on tumor progression. Urology. 2004; 63:682–686.38. Kang HW, Tchey DU, Yan C, Kim WT, Kim YJ, Yun SJ, et al. The predictive value of GSTT1 polymorphisms in predicting the early response to induction BCG therapy in patients with non-muscle invasive bladder cancer. Urol Oncol. 2014; 32:458–465.39. Kim YJ, Ha YS, Kim SK, Yoon HY, Lym MS, Kim MJ, et al. Gene signatures for the prediction of response to Bacillus Calmette-Guerin immunotherapy in primary pT1 bladder cancers. Clin Cancer Res. 2010; 16:2131–2137.40. Zuiverloon TC, Nieuweboer AJ, Vekony H, Kirkels WJ, Bangma CH, Zwarthoff EC. Markers predicting response to bacillus Calmette-Guérin immunotherapy in high-risk bladder cancer patients: a systematic review. Eur Urol. 2012; 61:128–145.41. Cai T, Nesi G, Mazzoli S, Meacci F, Tinacci G, Luciani LG, et al. Prediction of response to bacillus Calmette-Guérin treatment in non-muscle invasive bladder cancer patients through interleukin-6 and interleukin-10 ratio. Exp Ther Med. 2012; 4:459–464.42. Kamat AM, Briggman J, Urbauer DL, Svatek R, Nogueras Gonzalez GM, Anderson R, et al. Cytokine Panel for Response to Intravesical Therapy (CyPRIT): nomogram of changes in urinary cytokine levels predicts patient response to bacillus Calmette-Guérin. Eur Urol. 2016; 69:197–200.43. Lambert EH, Pierorazio PM, Olsson CA, Benson MC, McKiernan JM, Poon S. The increasing use of intravesical therapies for stage T1 bladder cancer coincides with decreasing survival after cystectomy. BJU Int. 2007; 100:33–36.44. Gupta A, Lotan Y, Bastian PJ, Palapattu GS, Karakiewicz PI, Raj GV, et al. Outcomes of patients with clinical T1 grade 3 urothelial cell bladder carcinoma treated with radical cystectomy. Urology. 2008; 71:302–307.45. Denzinger S, Fritsche HM, Otto W, Blana A, Wieland WF, Burger M. Early versus deferred cystectomy for initial high-risk pT1G3 urothelial carcinoma of the bladder: do risk factors define feasibility of bladder-sparing approach? Eur Urol. 2008; 53:146–152.46. Hautmann RE, de Petriconi RC, Volkmer BG. Lessons learned from 1,000 neobladders: the 90-day complication rate. J Urol. 2010; 184:990–994.47. Hautmann RE, Abol-Enein H, Davidsson T, Gudjonsson S, Hautmann SH, Holm HV, et al. ICUD-EAU International Consultation on Bladder Cancer 2012: Urinary diversion. Eur Urol. 2013; 63:67–80.48. Wiesner C, Pfitzenmaier J, Faldum A, Gillitzer R, Melchior SW, Thüroff JW. Lymph node metastases in non-muscle invasive bladder cancer are correlated with the number of transurethral resections and tumour upstaging at radical cystectomy. BJU Int. 2005; 95:301–305.49. Kitamura H, Kakehi Y. Treatment and management of high-grade T1 bladder cancer: what should we do after second TUR? Jpn J Clin Oncol. 2015; 45:315–322.50. Kunieda F, Kitamura H, Niwakawa M, Kuroiwa K, Shinohara N, Tobisu K, et al. Watchful waiting versus intravesical BCG therapy for high-grade pT1 bladder cancer with pT0 histology after second transurethral resection: Japan Clinical Oncology Group Study JCOG1019. Jpn J Clin Oncol. 2012; 42:1094–1098.51. Hautmann RE, Volkmer BG, Gust K. Quantification of the survival benefit of early versus deferred cystectomy in high-risk non-muscle invasive bladder cancer (T1 G3). World J Urol. 2009; 27:347–351.52. Jager W, Thomas C, Haag S, Hampel C, Salzer A, Thuroff JW, et al. Early vs delayed radical cystectomy for high-risk carcinoma not invading bladder muscle: delay of cystectomy reduces cancer-specific survival. BJU Int. 2011; 108(8 Pt 2):E284–E288.53. Badalato GM, Gaya JM, Hruby G, Patel T, Kates M, Sadeghi N, et al. Immediate radical cystectomy vs conservative management for high grade cT1 bladder cancer: is there a survival difference? BJU Int. 2012; 110:1471–1477.54. Sternberg IA, Keren Paz GE, Chen LY, Herr HW, Dalbagni G. Role of immediate radical cystectomy in the treatment of patients with residual T1 bladder cancer on restaging transurethral resection. BJU Int. 2013; 112:54–59.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrence and Progression of Stage T1 Bladder Tumor after Intravesical Bacillus Calmette-Guerin(BCG) Therapy
- A Clinical Efficacy of Intravesical Bacillus Calmette-Guerin Therapy of Stage T1 Bladder Cancer
- Bacillus Calmette-Guerin Intravesical Therapy in Superficial Bladder Cancer: The Early Experience of Comparison of 6 Week Course and Modified 6 3 Maintenance Therapy
- The Prognostic Parameters for Recurrence in the Superficial Bladder Cancer
- Recurrence According to Grade after BCG Intravesical Therapy in Stage T1 Bladder Cancer
