Yonsei Med J.
2018 Dec;59(10):1232-1239. 10.3349/ymj.2018.59.10.1232.
Single Ventilation during Cardiopulmonary Resuscitation Results in Better Neurological Outcomes in a Porcine Model of Cardiac Arrest
- Affiliations
-
- 1Department of Emergency Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea. chaemp@yonsei.ac.kr
- KMID: 2426338
- DOI: http://doi.org/10.3349/ymj.2018.59.10.1232
Abstract
- PURPOSE
Recent basic life support (BLS) guidelines recommend a 30:2 compression-to-ventilation ratio (CV2) or chest compression-only cardiopulmonary resuscitation (CC); however, there are inevitable risks of interruption of high-quality cardiopulmonary resuscitation (CPR) in CV2 and hypoxemia in CC. In this study, we compared the short-term outcomes among CC, CV2, and 30:1 CV ratio (CV1).
MATERIALS AND METHODS
In total, 42 pigs were randomly assigned to CC, CV1, or CV2 groups. After induction of ventricular fibrillation (VF), we observed pigs for 2 minutes without any intervention. Thereafter, BLS was started according to the assigned method and performed for 8 minutes. Defibrillation was performed after BLS and repeated every 2 minutes, followed by rhythm analysis. Advanced cardiac life support, including continuous chest compression with ventilation every 6 seconds and intravenous injection of 1 mg epinephrine every 4 minutes, was performed until the return of spontaneous circulation (ROSC) or 22 minutes after VF induction. Hemodynamic parameters and arterial blood gas profiles were compared among groups. ROSC, 24-hour survival, and neurologic outcomes were evaluated at 24 hours.
RESULTS
The hemodynamic parameters during CPR did not differ among the study groups. Partial pressure of oxygen in arterial blood and arterial oxygen saturation were lowest in the CC group, compared to those in the other groups, during the BLS period (p=0.002 and p < 0.001, respectively). The CV1 groups showed a significantly higher rate of favorable neurologic outcome (swine CPC 1 or 2) than the other groups (p=0.044).
CONCLUSION
CPR with CV1 could promote better neurologic outcome than CV2 and CC.
MeSH Terms
Figure
-

Fig. 1 Study protocol. VF, ventricular fibrillation; BLS, basic life support; ACLS, advanced cardiac life support; CC, chest compression-only CPR; CV1, CPR with 30:1 compression-to-ventilation ratio, CV2, CPR with 30:2 compression-to-ventilation ratio; ROSC, return of spontaneous circulation; CPC, cerebral performance category.
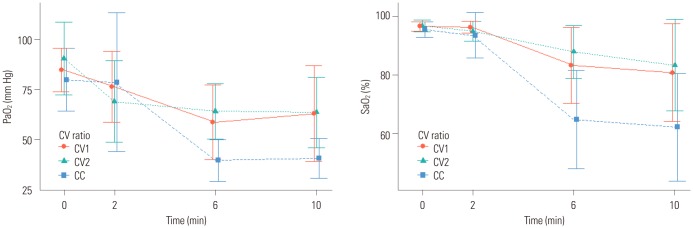
Fig. 2 Comparison of arterial oxygen parameters during basic life support. CV ratio, compression-to-ventilation ratio; CC, chest compression-only CPR; CV1, 30:1 CV ratio; CV2, 30:2 CV ratio.
Reference
-
1. Song KJ, Kim JB, Kim J, Kim C, Park SY, Lee CH, et al. Part 2. Adult basic life support: 2015 Korean Guidelines for Cardiopulmonary Resuscitation. Clin Exp Emerg Med. 2016; 3(Suppl):S10–S16. PMID: 27752642.
Article2. Travers AH, Perkins GD, Berg RA, Castren M, Considine J, Escalante R, et al. Part 3: Adult basic life support and automated external defibrillation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation. 2015; 132(16 Suppl 1):S51–S83. PMID: 26472859.
Article3. Perkins GD, Handley AJ, Koster RW, Castrén M, Smyth MA, Olasveengen T, et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation. 2015; 95:81–99. PMID: 26477420.4. Brenner BE, Van DC, Cheng D, Lazar EJ. Determinants of reluctance to perform CPR among residents and applicants: the impact of experience on helping behavior. Resuscitation. 1997; 35:203–211. PMID: 10203397.
Article5. Hew P, Brenner B, Kaufman J. Reluctance of paramedics and emergency medical technicians to perform mouth-to-mouth resuscitation. J Emerg Med. 1997; 15:279–284. PMID: 9258774.
Article6. Yeh ST, Cawley RJ, Aune SE, Angelos MG. Oxygen requirement during cardiopulmonary resuscitation (CPR) to effect return of spontaneous circulation. Resuscitation. 2009; 80:951–955. PMID: 19520479.
Article7. Dorph E, Wik L, Strømme TA, Eriksen M, Steen PA. Oxygen delivery and return of spontaneous circulation with ventilation: compression ratio 2:30 versus chest compressions only CPR in pigs. Resuscitation. 2004; 60:309–318. PMID: 15050764.8. Botran M, Lopez-Herce J, Urbano J, Solana MJ, Garcia A, Carrillo A. Chest compressions versus ventilation plus chest compressions: a randomized trial in a pediatric asphyxial cardiac arrest animal model. Intensive Care Med. 2011; 37:1873–1880. PMID: 21847647.
Article9. Fenici P, Idris AH, Lurie KG, Ursella S, Gabrielli A. What is the optimal chest compression-ventilation ratio? Curr Opin Crit Care. 2005; 11:204–211. PMID: 15928467.
Article10. Hostler D, Guimond G, Callaway C. A comparison of CPR delivery with various compression-to-ventilation ratios during two-rescuer CPR. Resuscitation. 2005; 65:325–328. PMID: 15919570.
Article11. Hüpfl M, Selig HF, Nagele P. Chest-compression-only versus standard cardiopulmonary resuscitation: a meta-analysis. Lancet. 2010; 376:1552–1557. PMID: 20951422.
Article12. Kleinman ME, Brennan EE, Goldberger ZD, Swor RA, Terry M, Bobrow BJ, et al. Part 5: Adult basic life support and cardiopulmonary resuscitation quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015; 132(18 Suppl 2):S414–S435. PMID: 26472993.13. Yannopoulos D, Tang W, Roussos C, Aufderheide TP, Idris AH, Lurie KG. Reducing ventilation frequency during cardiopulmonary resuscitation in a porcine model of cardiac arrest. Respir Care. 2005; 50:628–635. PMID: 15871757.14. Aufderheide TP, Sigurdsson G, Pirrallo RG, Yannopoulos D, McKnite S, von Briesen C, et al. Hyperventilation-induced hypotension during cardiopulmonary resuscitation. Circulation. 2004; 109:1960–1965. PMID: 15066941.
Article15. Spoormans I, Van Hoorenbeeck K, Balliu L, Jorens PG. Gastric perforation after cardiopulmonary resuscitation: review of the literature. Resuscitation. 2010; 81:272–280. PMID: 20064683.
Article16. Hwang SO, Kim SH, Kim H, Jang YS, Zhao PG, Lee KH, et al. Comparison of 15:1, 15:2, and 30:2 compression-to-ventilation ratios for cardiopulmonary resuscitation in a canine model of a simulated, witnessed cardiac arrest. Acad Emerg Med. 2008; 15:183–189. PMID: 18275449.
Article17. Cha KC, Kim YW, Kim TH, Jung WJ, Yook H, Choi E, et al. Comparison between 30:1 and 30:2 compression-to-ventilation ratios for cardiopulmonary resuscitation: are two ventilations necessary? Acad Emerg Med. 2015; 22:1261–1266. PMID: 26470011.
Article18. Berg RA, Otto CW, Kern KB, Sanders AB, Hilwig RW, Hansen KK, et al. High-dose epinephrine results in greater early mortality after resuscitation from prolonged cardiac arrest in pigs: a prospective, randomized study. Crit Care Med. 1994; 22:282–290. PMID: 8306688.
Article19. Hamel MB, Phillips R, Teno J, Davis RB, Goldman L, Lynn J, et al. Cost effectiveness of aggressive care for patients with nontraumatic coma. Crit Care Med. 2002; 30:1191–1196. PMID: 12072667.
Article20. Callaway CW, Donnino MW, Fink EL, Geocadin RG, Golan E, Kern KB, et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015; 132(18 Suppl 2):S465–S482. PMID: 26472996.21. Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, Böttiger BW, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008; 118:2452–2483. PMID: 18948368.22. Meaney PA, Bobrow BJ, Mancini ME, Christenson J, de Caen AR, Bhanji F, et al. Cardiopulmonary resuscitation quality: [corrected] improving cardiac resuscitation outcomes both inside and outside the hospital: a consensus statement from the American Heart Association. Circulation. 2013; 128:417–435. PMID: 23801105.23. Sanders AB, Kern KB, Berg RA, Hilwig RW, Heidenrich J, Ewy GA. Survival and neurologic outcome after cardiopulmonary resuscitation with four different chest compression-ventilation ratios. Ann Emerg Med. 2002; 40:553–562. PMID: 12447330.
Article24. Lurie KG, Zielinski T, McKnite S, Aufderheide T, Voelckel W. Use of an inspiratory impedance valve improves neurologically intact survival in a porcine model of ventricular fibrillation. Circulation. 2002; 105:124–129. PMID: 11772887.
Article25. Dorph E, Wik L, Strømme TA, Eriksen M, Steen PA. Quality of CPR with three different ventilation:compression ratios. Resuscitation. 2003; 58:193–201. PMID: 12909382.
Article26. Cavus E, Meybohm P, Bein B, Steinfath M, Pöppel A, Wenzel V, et al. Impact of different compression-ventilation ratios during basic life support cardiopulmonary resuscitation. Resuscitation. 2008; 79:118–124. PMID: 18586375.
Article27. Kwak SJ, Kim YM, Baek HJ, Kim SH, Yim HW. Chest compression quality, exercise intensity, and energy expenditure during cardiopulmonary resuscitation using compression-to-ventilation ratios of 15:1 or 30:2 or chest compression only: a randomized, crossover manikin study. Clin Exp Emerg Med. 2016; 3:148–157. PMID: 27752633.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- New Guideline of Pediatric Cardiopulmonary Resuscitation
- Role of extracorporeal cardiopulmonary resuscitation in adults
- A Prospective Study of the Epidemiology of Out-of-Hospital Pediatric Cardiopulmonary Arrest
- Thrombolytic Therapy during Cardiopulmonary Resuscitation in a Patient with Cardiac Arrest
- Cardiopulmonary Resuscitation: New Concept
