Clinical Diversity of Atopic Dermatitis: A Review of 5,000 Patients at a Single Institute
- Affiliations
-
- 1Department of Dermatology, Severance Hospital, Cutaneous Biology Research Institute, Yonsei University College of Medicine, Seoul, Korea. kwanglee@yuhs.ac
- KMID: 2413390
- DOI: http://doi.org/10.4168/aair.2017.9.2.158
Abstract
- PURPOSE
Atopic dermatitis (AD) is a chronic eczematous dermatitis that has a high prevalence and diverse clinical features. Although several hypotheses about its multifactorial pathogenesis have been suggested, the cause is not yet fully understood. A better understanding of the clinical features may helpful inelucidating the pathogenesis of AD.
METHODS
This retrospective study analyzed the questionnaires, medical charts, and laboratory examination results of 5,000 patients diagnosed with AD at a single tertiary hospital in Korea.
RESULTS
The demographics, allergic comorbidities, family history, severity, and treatment experiences of the patients were analyzed. Most of the patients were adults, 76.3% of whom were classified as havingan extrinsic type of AD. The mean eczema area and severity index (EASI) score was found to be 13.68, and adult patients were found to have higher severity than the other age groups. The anatomical involvements were different among the age groups, with more involvements of the head and neck in adults. The patients reported seasonal changes and stress as the factors that aggravated their symptoms the most. Topical steroids and oral cyclosporine were the most used medications at our clinic, whereas 10.1% of the patients underwent allergen-specific immunotherapy.
CONCLUSION
This analysis of 5,000 patients would lead to a better understanding of various subtypes and diverse clinical features of AD in Koreans. Distinct characteristics were observed among different age groups; thus, treatment strategies may need to be differentiated accordingly.
Keyword
MeSH Terms
Figure
-
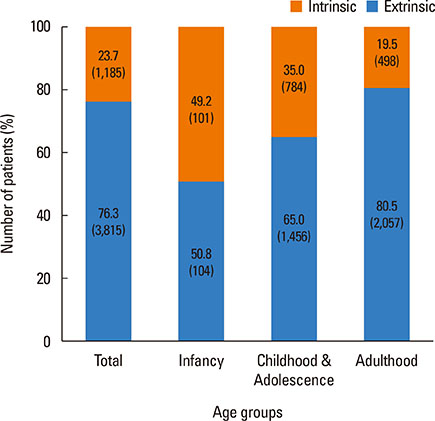
Fig. 1 The proportion of extrinsic and intrinsic types according to different age groups. The age groups were defined as follows: infancy ≤2 years old, childhood and adolescence >2 years old and ≤18 years old, and adulthood>18 years old. The intrinsic type was defined as a total IgE of <150 kU/L and with no sensitization to allergens, whereas the extrinsic type was defined as a total IgE of >150 kU/L or a positive sensitization in CAP immunoassay.
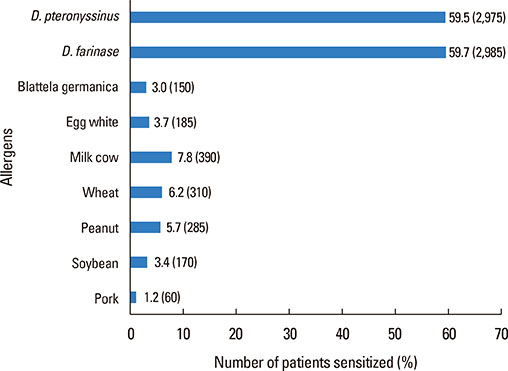
Fig. 2 Evaluation of sensitization to specific allergens in CAP immunoassay. D. pteronyssinus, Dermatophagoidespteronyssinus; D. farinae, Dermatophagoidesfarinae.
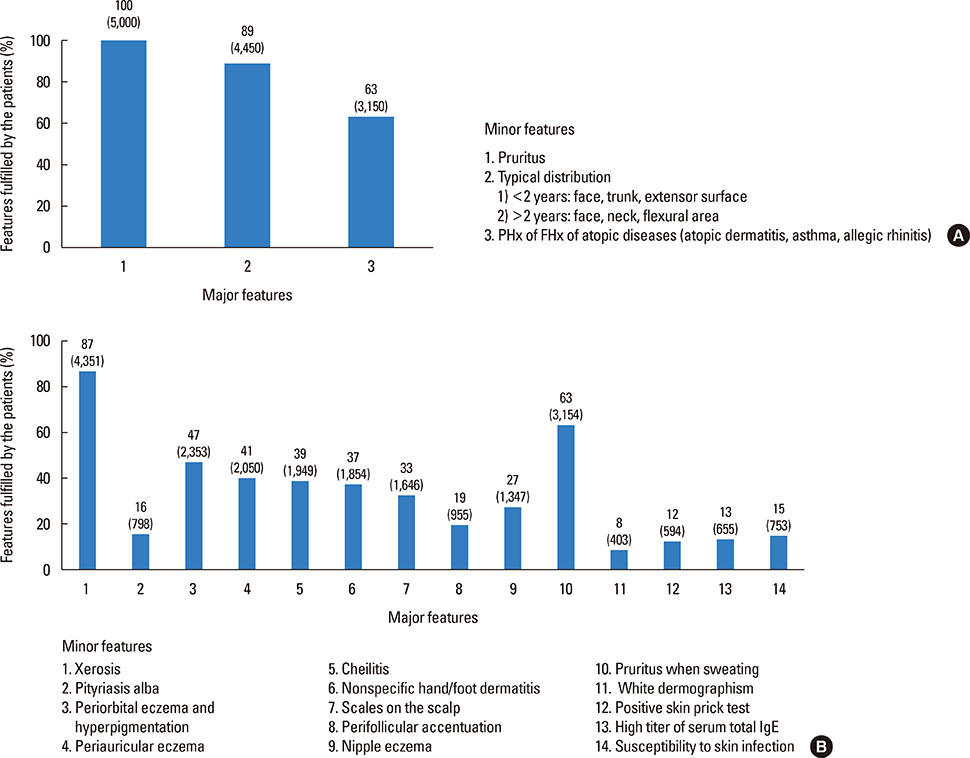
Fig. 3 The percentages of each fulfilled criterion of the (A) major features and (B) minor features of the diagnostic criteria. PHx, past history; FHx, family history.
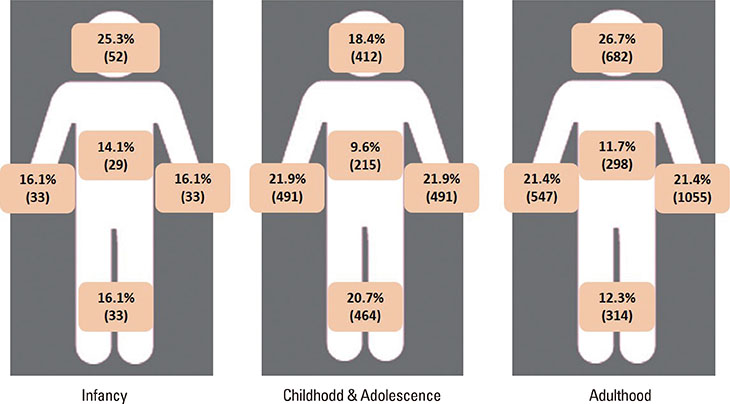
Fig. 4 Proportion of the involved parts of the body according to different age groups.The age groups are defined as follows: infancy ≤2 years old, childhood and adolescence >2 years old and ≤18 years old, adulthood >18 years old.

Fig. 5 Association of severity and age. (A) The patients of different age groups stratified by EASI scores into mild, moderate, and severe groups. (B) The differences of EASI scores between adult patients with onset before adulthood and those with adultonset. The age groups were defined as follows: infancy ≤2 years old, childhood and adolescence >2 years old and ≤18 years old, and adulthood >18 years old.The EASI scores ranged from 0 to 72, with the scores stratified as follows: mild <7, moderate ≥7 and <21, and severe ≥21. EASI, eczema area and severity index. *P<0.01.
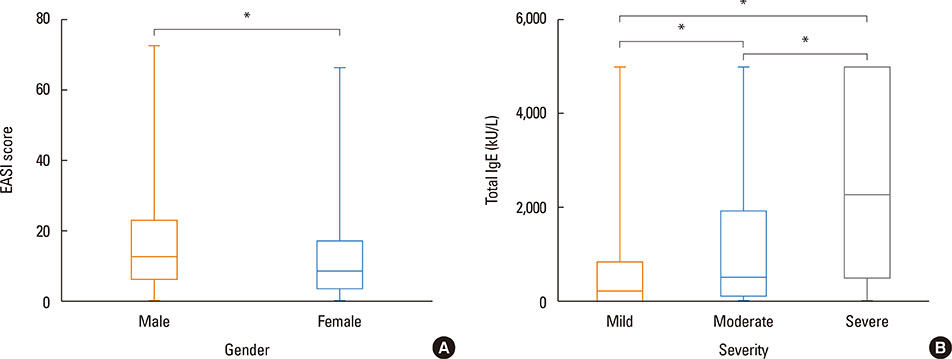
Fig. 6 (A) Comparison of EASI scores in male and female patients.(B)The association of totalIgE levels of different severity groups categorized by EASI scores. The EASI scores ranged from 0 to 72. The severity was stratified according to EASI scores as follows: mild <7, moderate ≥7 and<21, and severe ≥21. EASI, eczema area and severity index. *P<0.001.
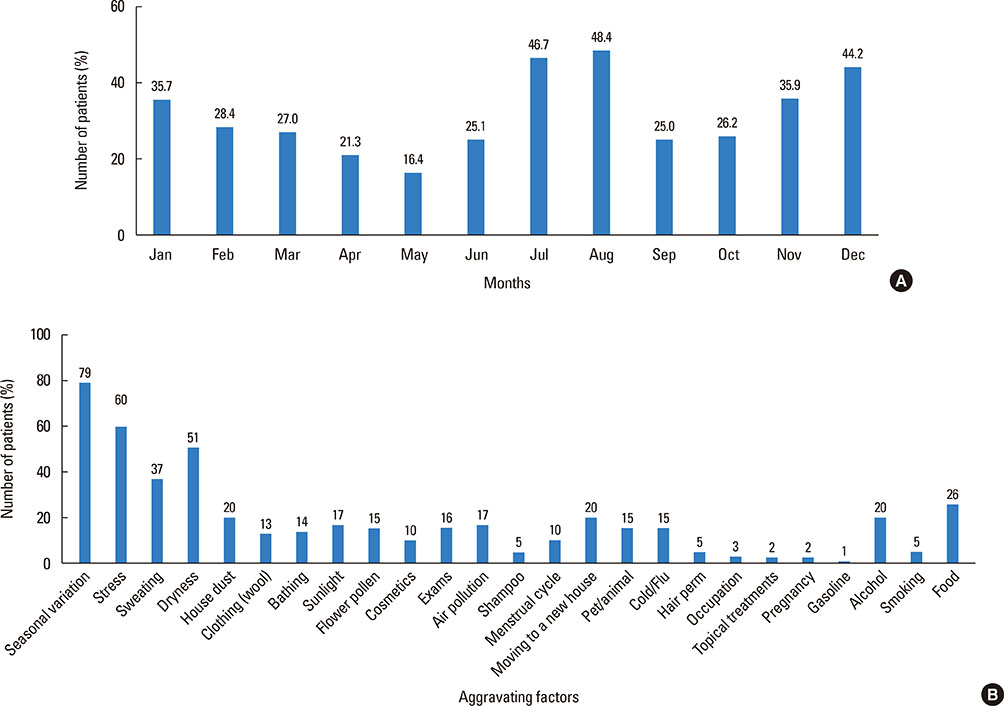
Fig. 7 (A) Aggravating factors. (B) Aggravation of symptoms according to months of the year assessed by using a questionnaire.
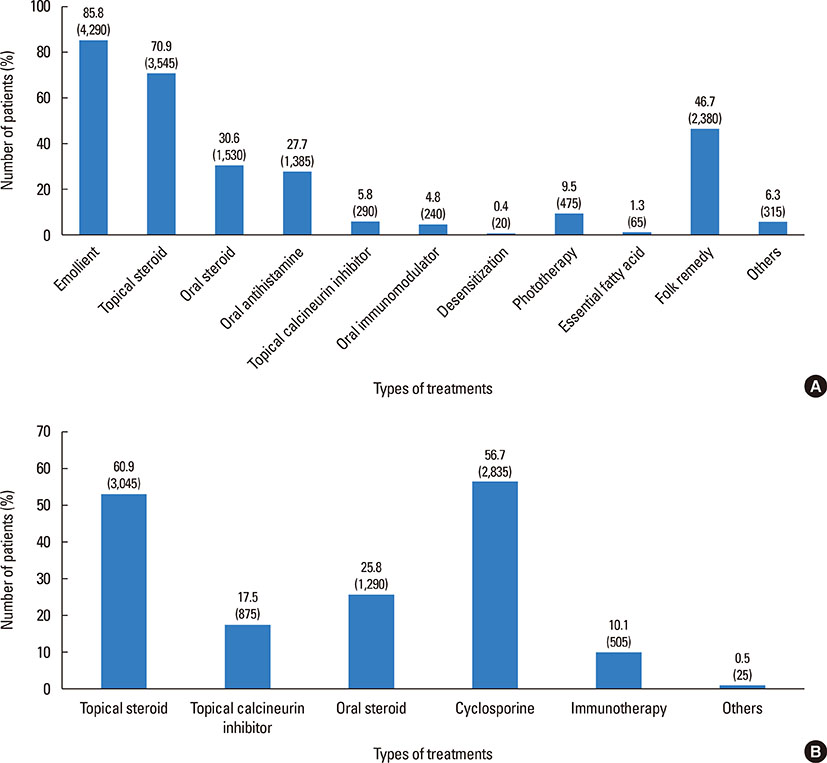
Fig. 8 List of the treatments that the patients have received (A) in the past and (B) at our clinic.
Reference
-
1. DaVeiga SP. Epidemiology of atopic dermatitis: a review. Allergy Asthma Proc. 2012; 33:227–234.2. Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015; 66:Suppl 1. 8–16.3. Kim C, Park KY, Ahn S, Kim DH, Li K, Kim DW, et al. Economic impact of atopic dermatitis in Korean patients. Ann Dermatol. 2015; 27:298–305.4. Peng W, Novak N. Pathogenesis of atopic dermatitis. Clin Exp Allergy. 2015; 45:566–574.5. Novak N, Leung DY. Advances in atopic dermatitis. Curr Opin Immunol. 2011; 23:778–783.6. Malajian D, Guttman-Yassky E. New pathogenic and therapeutic paradigms in atopic dermatitis. Cytokine. 2015; 73:311–318.7. Pugliarello S, Cozzi A, Gisondi P, Girolomoni G. Phenotypes of atopic dermatitis. J Dtsch Dermatol Ges. 2011; 9:12–20.8. Hanifin JM, Rajka G. Diagnostic features of atopic eczema. Acta Derm Venereol Suppl (Stockh). 1980; 92:44–47.9. Park YL, Kim HD, Kim KH, Kim MN, Kim JW, Ro YS, et al. Report from ADRG: a study on the diagnostic criteria of Korean atopic dermatitis. Korean J Dermatol. 2006; 44:659–663.10. Hanifin JM, Thurston M, Omoto M, Cherill R, Tofte SJ, Graeber M, et al. The eczema area and severity index (EASI): assessment of reliability in atopic dermatitis. EASI Evaluator Group. Exp Dermatol. 2001; 10:11–18.11. Leshem YA, Hajar T, Hanifin JM, Simpson EL. What the Eczema Area and Severity Index score tells us about the severity of atopic dermatitis: an interpretability study. Br J Dermatol. 2015; 172:1353–1357.12. Schmid-Grendelmeier P, Simon D, Simon HU, Akdis CA, Wüthrich B. Epidemiology, clinical features, and immunology of the “intrinsic” (non-IgE-mediated) type of atopic dermatitis (constitutional dermatitis). Allergy. 2001; 56:841–849.13. Tokura Y. Extrinsic and intrinsic types of atopic dermatitis. J Dermatol Sci. 2010; 58:1–7.14. Lee JH, Han KD, Kim KM, Park YG, Lee JY, Park YM. Prevalence of atopic dermatitis in Korean children based on data from the 2008–2011 Korean National Health and Nutrition Examination Survey. Allergy Asthma Immunol Res. 2016; 8:79–83.15. Wananukul S, Chatproedprai S, Tempark T, Phuthongkamt W, Chatchatee P. The natural course of childhood atopic dermatitis: a retrospective cohort study. Asian Pac J Allergy Immunol. 2015; 33:161–168.16. Pyun BY. Natural history and risk factors of atopic dermatitis in children. Allergy Asthma Immunol Res. 2015; 7:101–105.17. Chung Y, Kwon JH, Kim J, Han Y, Lee SI, Ahn K. Retrospective analysis of the natural history of atopic dermatitis occurring in the first year of life in Korean children. J Korean Med Sci. 2012; 27:723–728.18. Cosickic A, Skokic F, Colic-Hadzic B, Jahic M. Clinical characteristics and estimation severity of the atopic dermatitis in children. Med Arh. 2010; 64:178–182.19. Kulthanan K, Samutrapong P, Jiamton S, Tuchinda P. Adult-onset atopic dermatitis: a cross-sectional study of natural history and clinical manifestation. Asian Pac J Allergy Immunol. 2007; 25:207–214.20. Čelakovská J, Ettlerová K, Ettler K, Vaněčková J, Bukač J. Sensitization to aeroallergens in atopic dermatitis patients: association with concomitant allergic diseases. J Eur Acad Dermatol Venereol. 2015; 29:1500–1505.21. Darsow U, Laifaoui J, Kerschenlohr K, Wollenberg A, Przybilla B, Wüthrich B, et al. The prevalence of positive reactions in the atopy patch test with aeroallergens and food allergens in subjects with atopic eczema: a European multicenter study. Allergy. 2004; 59:1318–1325.22. Garritsen FM, ter Haar NM, Spuls PI. House dust mite reduction in the management of atopic dermatitis.A critically appraised topic. Br J Dermatol. 2013; 168:688–691.23. Banerjee S, Resch Y, Chen KW, Swoboda I, Focke-Tejkl M, Blatt K, et al. Der p 11 is a major allergen for house dust mite-allergic patients suffering from atopic dermatitis. J Invest Dermatol. 2015; 135:102–109.24. Kiiski V, Karlsson O, Remitz A, Reitamo S. High serum total IgE predicts poor long-term outcome in atopic dermatitis. Acta Derm Venereol. 2015; 95:943–947.25. Flohr C, Johansson SG, Wahlgren CF, Williams H. How atopic is atopic dermatitis? J Allergy Clin Immunol. 2004; 114:150–158.26. Kulthanan K, Boochangkool K, Tuchinda P, Chularojanamontri L. Clinical features of the extrinsic and intrinsic types of adult-onset atopic dermatitis. Asia Pac Allergy. 2011; 1:80–86.27. Ott H, Stanzel S, Ocklenburg C, Merk HF, Baron JM, Lehmann S. Total serum IgE as a parameter to differentiate between intrinsic and extrinsic atopic dermatitis in children. Acta Derm Venereol. 2009; 89:257–261.28. Brenninkmeijer EE, Spuls PI, Legierse CM, Lindeboom R, Smitt JH, Bos JD. Clinical differences between atopic and atopiform dermatitis. J Am Acad Dermatol. 2008; 58:407–414.29. Choi SJ, Song MG, Sung WT, Lee DY, Lee JH, Lee ES, et al. Comparison of transepidermal water loss, capacitance and pH values in the skin between intrinsic and extrinsic atopic dermatitis patients. J Korean Med Sci. 2003; 18:93–96.30. Fölster-Holst R, Pape M, Buss YL, Christophers E, Weichenthal M. Low prevalence of the intrinsic form of atopic dermatitis among adult patients. Allergy. 2006; 61:629–632.31. Park JH, Choi YL, Namkung JH, Kim WS, Lee JH, Park HJ, et al. Characteristics of extrinsic vs intrinsic atopic dermatitis in infancy: correlations with laboratory variables. Br J Dermatol. 2006; 155:778–783.32. Kanwar AJ, Narang T. Adult onset atopic dermatitis: Under-recognized or under-reported? Indian Dermatol Online J. 2013; 4:167–171.33. Noh S, Park CO, Bae JM, Lee J, Shin JU, Hong CS, et al. Lower vitamin D status is closely correlated with eczema of the head and neck. J Allergy Clin Immunol. 2014; 133:1767–1770.e6.34. Orfali RL, Shimizu MM, Takaoka R, Zaniboni MC, Ishizaki AS, Costa AA, et al. Atopic dermatitis in adults: clinical and epidemiological considerations. Rev Assoc Med Bras (1992). 2013; 59:270–275.35. Kim MJ, Kang TW, Cho EA, Kim HS, Min JA, Park H, et al. Prevalence of atopic dermatitis among Korean adults visiting health service center of the Catholic Medical Center in Seoul Metropolitan Area, Korea. J Korean Med Sci. 2010; 25:1828–1830.36. Laske N, Niggemann B. Does the severity of atopic dermatitis correlate with serum IgElevels? Pediatr Allergy Immunol. 2004; 15:86–88.37. Cowan MA. Nummular eczema. A review, follow-up and analysis of a series of 325 cases. Acta Derm Venereol. 1961; 41:453–460.38. Iking A, Grundmann S, Chatzigeorgakidis E, Phan NQ, Klein D, Ständer S. Prurigo as a symptom of atopic and non-atopic diseases: aetiological survey in a consecutive cohort of 108 patients. J Eur Acad Dermatol Venereol. 2013; 27:550–557.39. Leung DY. Why is eczema herpeticum unexpectedly rare? Antiviral Res. 2013; 98:153–157.40. Beck LA, Boguniewicz M, Hata T, Schneider LC, Hanifin J, Gallo R, et al. Phenotype of atopic dermatitis subjects with a history of eczema herpeticum. J Allergy ClinImmunol. 2009; 124:260–269. 269.e1–269.e7.41. Williams JR, Burr ML, Williams HC. Factors influencing atopic dermatitis-a questionnaire survey of schoolchildren's perceptions. Br J Dermatol. 2004; 150:1154–1161.42. Byremo G, Rød G, Carlsen KH. Effect of climatic change in children with atopic eczema. Allergy. 2006; 61:1403–1410.43. Engebretsen KA, Johansen JD, Kezic S, Linneberg A, Thyssen JP. The effect of environmental humidity and temperature on skin barrier function and dermatitis. J Eur Acad Dermatol Venereol. 2016; 30:223–249.44. Lee J, Park CO, Lee KH. Specific immunotherapy in atopic dermatitis. Allergy Asthma Immunol Res. 2015; 7:221–229.45. Bae JM, Choi YY, Park CO, Chung KY, Lee KH. Efficacy of allergen-specific immunotherapy for atopic dermatitis: a systematic review and meta-analysis of randomized controlled trials. J Allergy Clin Immunol. 2013; 132:110–117.46. Nahm DH, Kim ME, Kwon B, Cho SM, Ahn A. Clinical Efficacy of Subcutaneous Allergen Immunotherapy in Patients with Atopic Dermatitis. Yonsei Med J. 2016; 57:1420–1426.47. Lee J, Lee H, Noh S, Bae BG, Shin JU, Park CO, et al. Retrospective Analysis on the effects of house dust mite specific immunotherapy for more than 3 years in atopic dermatitis. Yonsei Med J. 2016; 57:393–398.48. Werfel T, Breuer K, Ruéff F, Przybilla B, Worm M, Grewe M, et al. Usefulness of specific immunotherapy in patients with atopic dermatitis and allergic sensitization to house dust mites: a multi-centre, randomized, dose-response study. Allergy. 2006; 61:202–205.49. Lee JH, Son SW, Cho SH. A comprehensive review of the treatment of atopic eczema. Allergy Asthma Immunol Res. 2016; 8:181–190.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Measurement of Atopic Dermatitis Disability
- Serum IgE Level in Patients of Atopic Dermatitis and Atopic Dermatitis with Molluscum Contagiosum
- Atopic dermatitis
- Clinical Characteristics of Lichen Amyloidosis Associated with Atopic Dermatitis: A Single Center, Retrospective Study
- Age-related Changes in the Frequency of Intrinsic and Extrinsic Atopic Dermatitis: A Single-center Retrospective Study
