J Rheum Dis.
2017 Aug;24(4):185-191. 10.4078/jrd.2017.24.4.185.
Augmentation Index in Connective Tissue Diseases
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea.
- 2Division of Rheumatology, Department of Internal Medicine, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea. valgom@naver.com
- KMID: 2389059
- DOI: http://doi.org/10.4078/jrd.2017.24.4.185
Abstract
- Atherosclerosis and its complications are often reported in patients with connective tissue diseases (CTDs) showing chronic inflammation. Traditional cardiovascular risk factors do not account for accelerated atherosclerosis in patients with CTDs. Inflammation, although non-traditional, is considered one of the risk factors for endothelial dysfunction, atrial stiffness, and atherosclerosis. Therefore, it is essential to evaluate other risk factors for cardiovascular disease (CVD) in patients with CTDs. The interest in pulse wave analysis (PWA) is growing because of its predictive value for CVD. The arterial pressure waveform is a composite of an incidental wave produced by a ventricular contraction and a reflected wave. The wave reflection can be quantified using the augmentation index (AIx); it is defined as the difference between the inflection and peak systolic pressure, and expressed as a percentage of the pulse pressure. The PWA is represented by AIx. Risk score systems, such as the Framingham scoring system, were correlated with AIx. Many studies have analyzed the ability of the AIx to predict the CAD severity in the general population. In patients with CTDs, the AIx was found to increase compared to a healthy control group. The AIx was related to the activity of CTDs. The treatment for inflammation appeared to improve the AIx in some CTDs. Although more studies will be needed to obtain conclusive evidence, AIx is expected to be a prognostic factor or a risk factor for CVD in patients with CTDs.
MeSH Terms
Figure
-
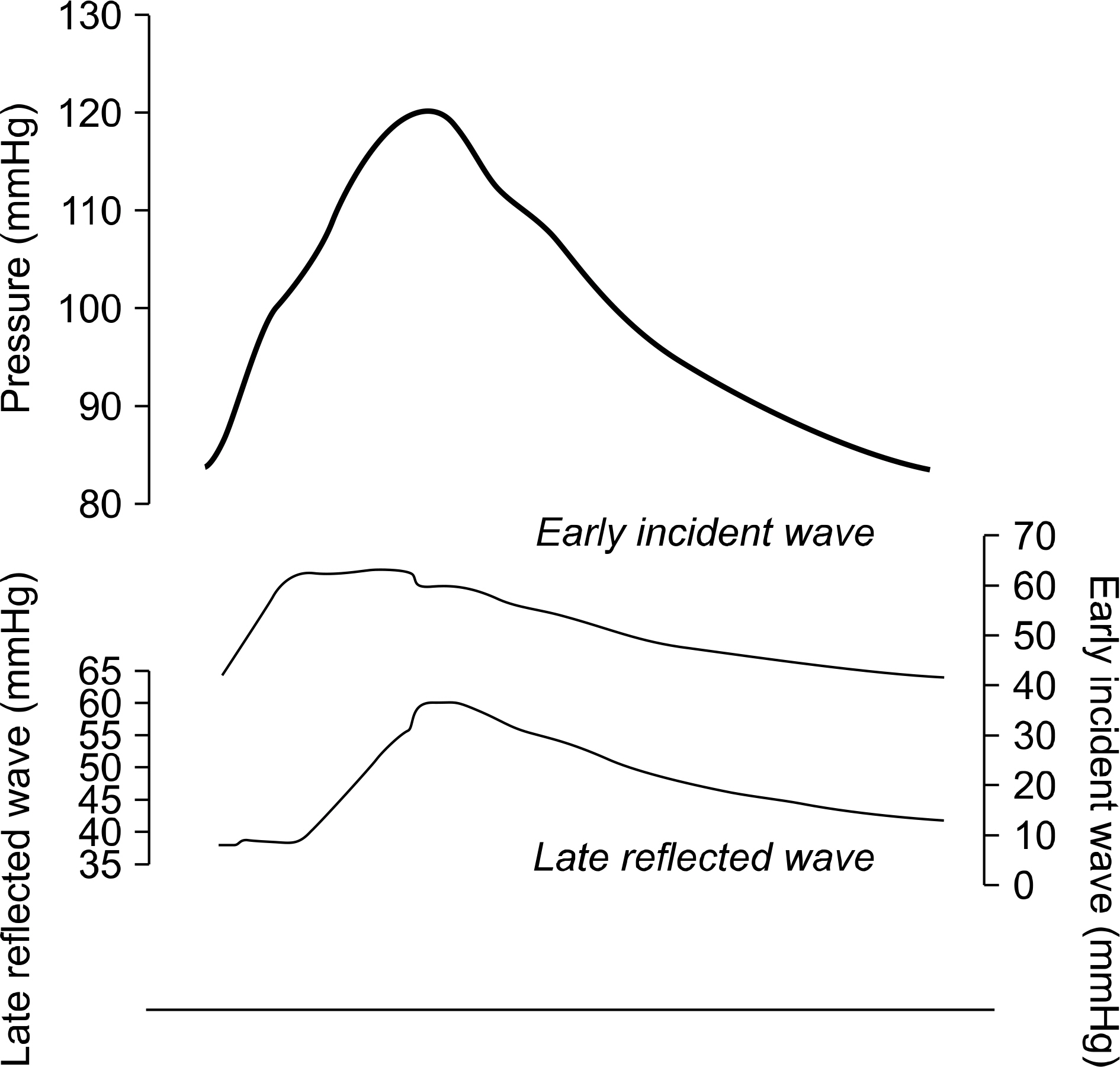
Figure 1. Central aortic pressure using SphygmoCor (Atcor Medical, Sydney, Australia) by applanating the left radial artery was separated into early incident wave and late reflected wave through the formula by central aortic flow using a Vivid 7 system (GE Vingmed, Horten, Norway) with a 3.5 MHz transducer.
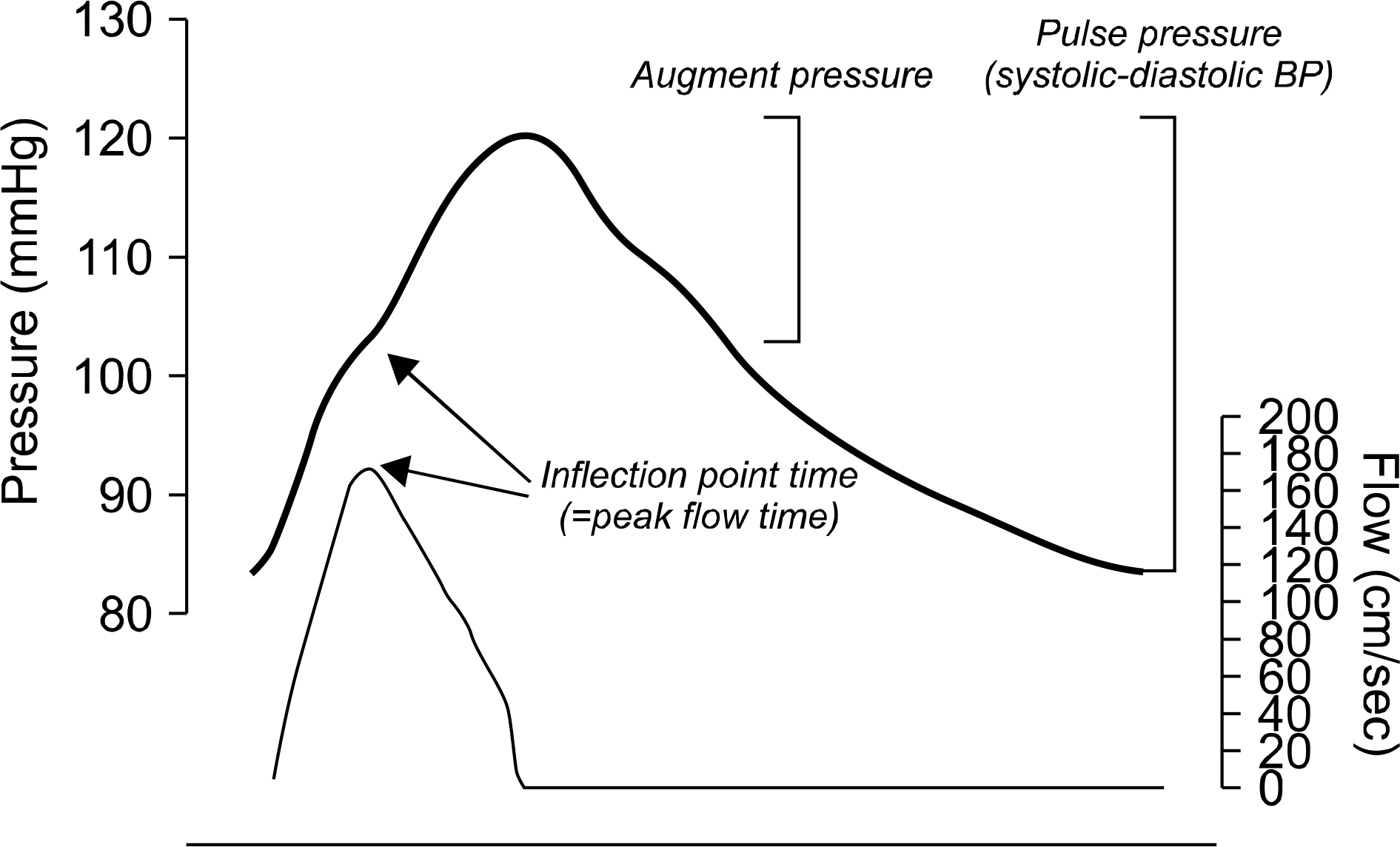
Figure 2. Augmentation index is defined as the ratio of augment pressure and pulse pressure and is usually expressed as a percentage. The inflection point indicates the beginning up-stroke of the reflected wave. The inflection point time is equal to the peak flow time.
Reference
-
1. D'Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008; 117:743–53.2. Safar ME, Blacher J, Jankowski P. Arterial stiffness, pulse pressure, and cardiovascular disease-is it possible to break the vicious circle? Atherosclerosis. 2011; 218:263–71.
Article3. Szodoray P, Timar O, Veres K, Der H, Szomjak E, Lakos G, et al. TH1/TH2 imbalance, measured by circulating and in-tracytoplasmic inflammatory cytokines–immunological alterations in acute coronary syndrome and stable coronary artery disease. Scand J Immunol. 2006; 64:336–44.4. Ross R. Atherosclerosis is an inflammatory disease. Am Heart J. 1999; 138:S419–20.
Article5. Shoenfeld Y, Gerli R, Doria A, Matsuura E, Cerinic MM, Ronda N, et al. Accelerated atherosclerosis in autoimmune rheumatic diseases. Circulation. 2005; 112:3337–47.
Article6. Choi CU, Park CG. Future trends in measuring blood pressure: Central pressure, pulse wave velocity, and pulse wave analysis. Korean J Med. 2009; 76:389–97.7. Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013; 34:2159–219.8. Staessen JA, Gasowski J, Wang JG, Thijs L, Den Hond E, Boissel JP, et al. Risks of untreated and treated isolated systolic hypertension in the elderly: meta-analysis of outcome trials. Lancet. 2000; 355:865–72.
Article9. Weber T, Auer J, O'Rourke MF, Kvas E, Lassnig E, Berent R, et al. Arterial stiffness, wave reflections, and the risk of coronary artery disease. Circulation. 2004; 109:184–9.
Article10. O'Rourke MF, Mancia G. Arterial stiffness. J Hypertens. 1999; 17:1–4.11. Asanuma Y, Oeser A, Shintani AK, Turner E, Olsen N, Fazio S, et al. Premature coronary-artery atherosclerosis in systemic lupus erythematosus. N Engl J Med. 2003; 349:2407–15.
Article12. Manzi S, Meilahn EN, Rairie JE, Conte CG, Medsger TA Jr, Jansen-McWilliams L, et al. Age-specific incidence rates of myocardial infarction and angina in women with systemic lupus erythematosus: comparison with the Framingham Study. Am J Epidemiol. 1997; 145:408–15.
Article13. Ngian GS, Sahhar J, Proudman SM, Stevens W, Wicks IP, Van Doornum S. Prevalence of coronary heart disease and cardiovascular risk factors in a national cross-sectional cohort study of systemic sclerosis. Ann Rheum Dis. 2012; 71:1980–3.
Article14. Youssef P, Brama T, Englert H, Bertouch J. Limited scleroderma is associated with increased prevalence of macro-vascular disease. J Rheumatol. 1995; 22:469–72.15. Pujades-Rodriguez M, Duyx B, Thomas SL, Stogiannis D, Rahman A, Smeeth L, et al. Rheumatoid arthritis and incidence of twelve initial presentations of cardiovascular disease: a population record-linkage cohort study in England. PLoS One. 2016; 11:e0151245.
Article16. Aviña-Zubieta JA, Abrahamowicz M, Choi HK, Rahman MM, Sylvestre MP, Esdaile JM, et al. Risk of cerebrovascular disease associated with the use of glucocorticoids in patients with incident rheumatoid arthritis: a population-based study. Ann Rheum Dis. 2011; 70:990–5.
Article17. Nakanishi N, Okamoto M, Yoshida H, Matsuo Y, Suzuki K, Tatara K. Serum uric acid and risk for development of hypertension and impaired fasting glucose or Type II diabetes in Japanese male office workers. Eur J Epidemiol. 2003; 18:523–30.
Article18. Shankar A, Klein R, Klein BE, Nieto FJ. The association between serum uric acid level and long-term incidence of hypertension: Population-based cohort study. J Hum Hypertens. 2006; 20:937–45.
Article19. Masuo K, Kawaguchi H, Mikami H, Ogihara T, Tuck ML. Serum uric acid and plasma norepinephrine concentrations predict subsequent weight gain and blood pressure elevation. Hypertension. 2003; 42:474–80.
Article20. Essex MN, Hopps M, Bienen EJ, Udall M, Mardekian J, Makinson GT. Evaluation of the relationship between serum uric acid levels and cardiovascular events in patients with gout: a retrospective analysis using electronic medical record data. J Clin Rheumatol. 2017; 23:160–6.21. Pagidipati NJ, Hess CN, Clare RM, Akerblom A, Tricoci P, Wojdyla D, et al. An examination of the relationship between serum uric acid level, a clinical history of gout, and cardiovascular outcomes among patients with acute coronary syndrome. Am Heart J. 2017; 187:53–61.
Article22. Grimaldi-Bensouda L, Alpérovitch A, Aubrun E, Danchin N, Rossignol M, Abenhaim L, et al. Impact of allopurinol on risk of myocardial infarction. Ann Rheum Dis. 2015; 74:836–42.
Article23. Schieir O, Tosevski C, Glazier RH, Hogg-Johnson S, Badley EM. Incident myocardial infarction associated with major types of arthritis in the general population: a systematic review and meta-analysis. Ann Rheum Dis. 2017; 76:1396–404.
Article24. Man A, Zhu Y, Zhang Y, Dubreuil M, Rho YH, Peloquin C, et al. The risk of cardiovascular disease in systemic sclerosis: a population-based cohort study. Ann Rheum Dis. 2013; 72:1188–93.
Article25. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005; 352:1685–95.
Article26. Hunt BJ. The endothelium in atherogenesis. Lupus. 2000; 9:189–93.
Article27. Lopez LR, Simpson DF, Hurley BL, Matsuura E. OxLDL/be-ta2GPI complexes and autoantibodies in patients with systemic lupus erythematosus, systemic sclerosis, and anti-phospholipid syndrome: pathogenic implications for vascular involvement. Ann N Y Acad Sci. 2005; 1051; 313–22.28. Lippi G, Caramaschi P, Montagnana M, Salvagno GL, Volpe A, Guidi G. Lipoprotein[a] and the lipid profile in patients with systemic sclerosis. Clin Chim Acta. 2006; 364:345–8.
Article29. Kanellis J, Watanabe S, Li JH, Kang DH, Li P, Nakagawa T, et al. Uric acid stimulates monocyte chemoattractant protein-1 production in vascular smooth muscle cells via mi-togen-activated protein kinase and cyclooxygenase-2. Hypertension. 2003; 41:1287–93.
Article30. Kelly R, Hayward C, Avolio A, O'Rourke M. Noninvasive determination of age-related changes in the human arterial pulse. Circulation. 1989; 80:1652–9.
Article31. Choi J, Kim SY, Joo SJ, Kim KS. Augmentation index is associated with coronary revascularization in patients with high Framingham risk scores: a hospital-based observational study. BMC Cardiovasc Disord. 2015; 15:131.
Article32. Hayashi T, Nakayama Y, Tsumura K, Yoshimaru K, Ueda H. Reflection in the arterial system and the risk of coronary heart disease. Am J Hypertens. 2002; 15:405–9.
Article33. Nürnberger J, Keflioglu-Scheiber A, Opazo Saez AM, Wenzel RR, Philipp T, Schäfers RF. Augmentation index is associated with cardiovascular risk. J Hypertens. 2002; 20:2407–14.
Article34. Soltész P, Dér H, Kerekes G, Szodoray P, Szücs G, Dankó K, et al. A comparative study of arterial stiffness, flow-mediated vasodilation of the brachial artery, and the thickness of the carotid artery intima-media in patients with systemic autoimmune diseases. Clin Rheumatol. 2009; 28:655–62.
Article35. Ambrosino P, Tasso M, Lupoli R, Di Minno A, Baldassarre D, Tremoli E, et al. Non-invasive assessment of arterial stiffness in patients with rheumatoid arthritis: a systematic review and meta-analysis of literature studies. Ann Med. 2015; 47:457–67.
Article36. Sacre K, Escoubet B, Pasquet B, Chauveheid MP, Zennaro MC, Tubach F, et al. Increased arterial stiffness in systemic lupus erythematosus (SLE) patients at low risk for cardiovascular disease: a cross-sectional controlled study. PLoS One. 2014; 9:e94511.
Article37. Tsifetaki N, Georgiadis AN, Alamanos Y, Fanis S, Argyropoulou MI, Drosos AA. Subclinical atherosclerosis in scleroderma patients. Scand J Rheumatol. 2010; 39:326–9.
Article38. Peled N, Shitrit D, Fox BD, Shlomi D, Amital A, Bendayan D, et al. Peripheral arterial stiffness and endothelial dysfunction in idiopathic and scleroderma associated pulmonary arterial hypertension. J Rheumatol. 2009; 36:970–5.
Article39. Barbulescu AL, Vreju F, Cojocaru-Gofita IR, Musetescu AE, Ciurea PL. Impaired arterial stiffness in systemic lupus erty-thematosus – correlations with inflammation markers. Curr Health Sci J. 2012; 38:61–5.40. Shang Q, Tam LS, Li EK, Yip GW, Yu CM. Increased arterial stiffness correlated with disease activity in systemic lupus erythematosus. Lupus. 2008; 17:1096–102.
Article41. ESH/ESC Task Force for the Management of Arterial Hypertension. 2013 Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J Hypertens. 2013; 31:1925–38.42. Wu GC, Liu HR, Leng RX, Li XP, Li XM, Pan HF, et al. Subclinical atherosclerosis in patients with systemic lupus erythematosus: A systemic review and meta-analysis. Autoimmun Rev. 2016; 15:22–37.
Article43. Timár O, Soltész P, Szamosi S, Dér H, Szántó S, Szekanecz Z, et al. Increased arterial stiffness as the marker of vascular involvement in systemic sclerosis. J Rheumatol. 2008; 35:1329–33.44. Piccione MC, Bagnato G, Zito C, Di Bella G, Caliri A, Catalano M, et al. Early identification of vascular damage in patients with systemic sclerosis. Angiology. 2011; 62:338–43.
Article45. Choi JH, Joo SJ, Kim J. Determining the necessity for right heart catheterization in pulmonary hypertension associated with connective tissue diseases assessed by echocardiography. Int J Rheum Dis. 2016; 19:65–73.
Article46. Vlachopoulos C, Gravos A, Georgiopoulos G, Terentes-Printzios D, Ioakeimidis N, Vassilopoulos D, et al. The effect of TNF-a antagonists on aortic stiffness and wave reflections: a meta-analysis. Clin Rheumatol. 2017 May 8; [Epub].DOI: DOI: 10.1007/s10067-017-3657-y.
Article47. Gagliardi AC, Miname MH, Santos RD. Uric acid: A marker of increased cardiovascular risk. Atherosclerosis. 2009; 202:11–7.
Article48. Deng G, Qiu Z, Li D, Fang Y, Zhang S. Effects of allopurinol on arterial stiffness: a meta-analysis of randomized controlled trials. Med Sci Monit. 2016; 22:1389–97.
Article49. Elsurer R, Afsar B. Serum uric acid and arterial stiffness in hypertensive chronic kidney disease patients: sex-specific variations. Blood Press Monit. 2014; 19:271–9.50. Gómez-Marcos MA, Recio-Rodríguez JI, Patino-Alonso MC, Agudo-Conde C, Rodríguez-Sánchez E, Gómez-Sánchez L, et al. Relationship between uric acid and vascular structure and function in hypertensive patients and sex-related differences. Am J Hypertens. 2013; 26:599–607.51. Vlachopoulos C, Xaplanteris P, Vyssoulis G, Bratsas A, Baou K, Tzamou V, et al. Association of serum uric acid level with aortic stiffness and arterial wave reflections in newly diagnosed, never-treated hypertension. Am J Hypertens. 2011; 24:33–9.
Article52. Protogerou AD, Achimastos A, Vlachopoulos C, Stamatelopoulos KS, Papaioannou TG, Papamichael CM, et al. Reduced pressure wave reflections in patients with active clinical status of Adamantiades-Behcet disease. Hellenic J Cardiol. 2008; 49:408–14.53. Williams B, Lacy PS, Thom SM, Cruickshank K, Stanton A, Collier D, et al. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes: principal results of the Conduit Artery Function Evaluation (CAFE) study. Circulation. 2006; 113:1213–25.54. Morgan T, Lauri J, Bertram D, Anderson A. Effect of different antihypertensive drug classes on central aortic pressure. Am J Hypertens. 2004; 17:118–23.
Article55. Kanaki AI, Sarafidis PA, Georgianos PI, Kanavos K, Tziolas IM, Zebekakis PE, et al. Effects of low-dose atorvastatin on arterial stiffness and central aortic pressure augmentation in patients with hypertension and hypercholesterolemia.56. Van Doornum S, McColl G, Wicks IP. Atorvastatin reduces arterial stiffness in patients with rheumatoid arthritis. Ann Rheum Dis. 2004; 63:1571–5.
Article57. Barnes JN, Nualnim N, Sugawara J, Sommerlad SM, Renzi CP, Tanaka H. Arterial stiffening, wave reflection, and inflammation in habitually exercising systemic lupus erythematosus patients. Am J Hypertens. 2011; 24:1194–200.
Article58. Sfikakis PP, Papamichael C, Stamatelopoulos KS, Tousoulis D, Fragiadaki KG, Katsichti P, et al. Improvement of vascular endothelial function using the oral endothelin receptor antagonist bosentan in patients with systemic sclerosis. Arthritis Rheum. 2007; 56:1985–93.
Article59. Ng KP, Stringer SJ, Jesky MD, Yadav P, Athwal R, Dutton M, et al. Allopurinol is an independent determinant of improved arterial stiffness in chronic kidney disease: a cross-sectional study. PLoS One. 2014; 9:e91961.
Article60. Westerhof N, O'Rourke MF. Haemodynamic basis for the development of left ventricular failure in systolic hypertension and for its logical therapy. J Hypertens. 1995; 13:943–52.
Article61. Langenberg C, Hardy R, Breeze E, Kuh D, Wadsworth M. Influence of short stature on the change in pulse pressure, systolic and diastolic blood pressure from age 36 to 53 years: an analysis using multilevel models. Int J Epidemiol. 2005; 34:905–13.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pleural Effusion in Connective Tissue Diseases
- Ridge Augmentation Using Vascularized Interpositional Periosteal- Connective Tissue (VIP-CT) in Conjunction with Anterior Implant Placement in Maxilla: Report of Three Cases
- Diagnosis of protein losing enterpathy connective tissue diseases with Tc-human serum albumin(HSA)
- Early Detection of Pulmonary Hypertension in Connective Tissue Disease
- A Case of Trigeminal Neuropathy Associated with Mixed Connective Tissue Disease
