Unexpected Delayed Colon Perforation after the Endoscopic Submucosal Dissection with Snaring of a Laterally Spreading Tumor
- Affiliations
-
- 1Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jsbyeon@amc.seoul.kr
- KMID: 2380419
- DOI: http://doi.org/10.5946/ce.2015.48.6.570
Abstract
- Colonic perforation may occur as a complication of diagnostic and therapeutic colonoscopy. The risk factors for perforation after colorectal endoscopic submucosal dissection (ESD) include an inexperienced endoscopist, a large tumor size, and submucosal fibrosis. The mechanisms of perforation include unintended endoscopic resection/dissection and severe thermal injury. Here, we report a case of colon perforation that occurred after ESD with snaring of a laterally spreading tumor. The perforation was completely unexpected because there were no colorectal ESD-associated risk factors for perforation, deep dissection, or severe coagulation injury in our patient.
Figure
-
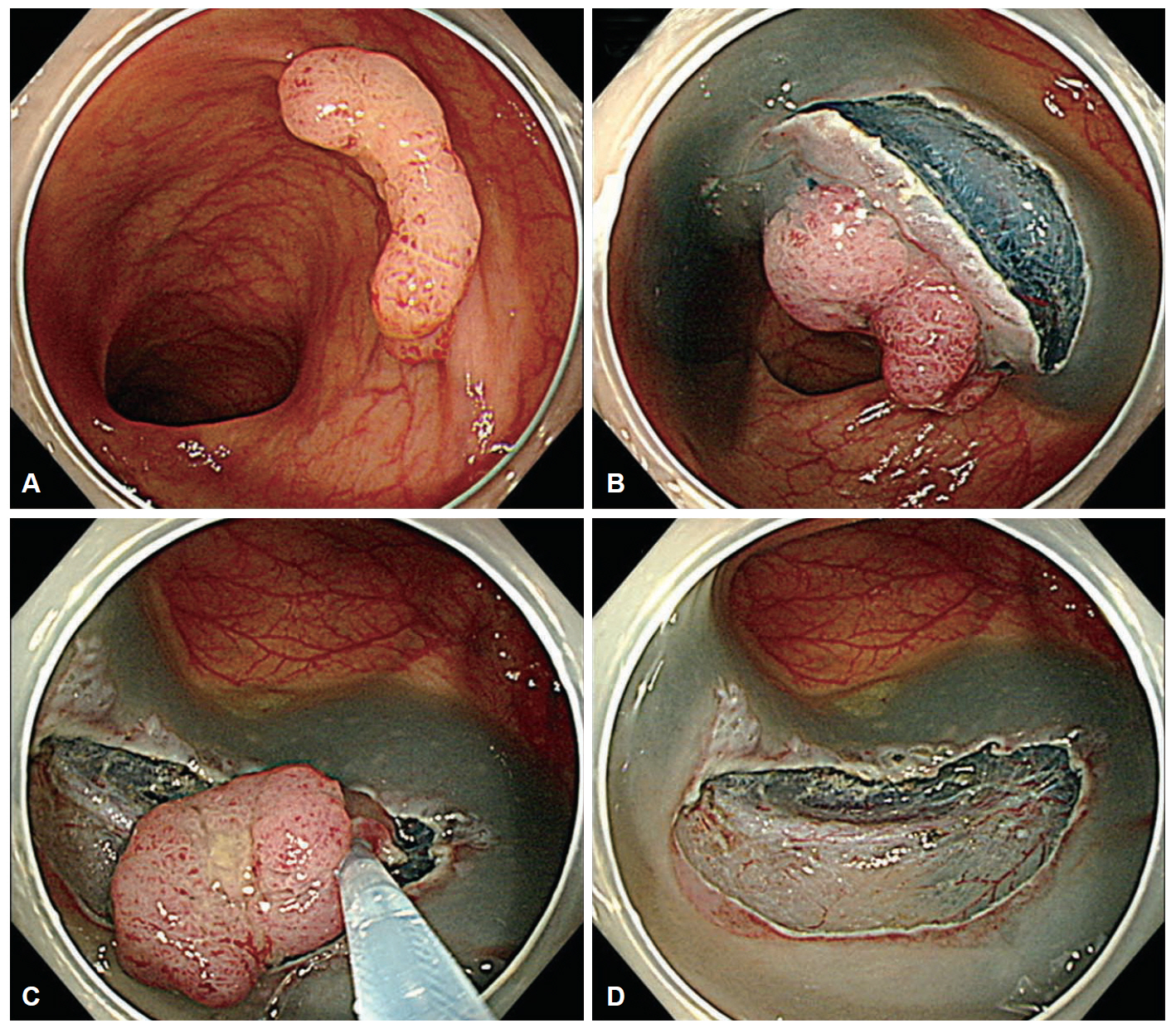
Fig. 1. (A) Nongranular laterally spreading tumor in the transverse colon. (B) Submucosal dissection was performed. (C) After partial endoscopic submucosal dissection (ESD), the lesion was removed en bloc by means of snaring. (D) En bloc resection was completed, and the post-ESD ulcer base was clean without bleeding, severe coagulation injury, or endoscopically evident perforation.

Fig. 2. (A, B) Pneumoperitoneum on simple abdominal imaging and abdominopelvic computed tomography (arrows). (C, D) Transverse colon wall thickening and irregularity (arrowheads) with pericolic free air.
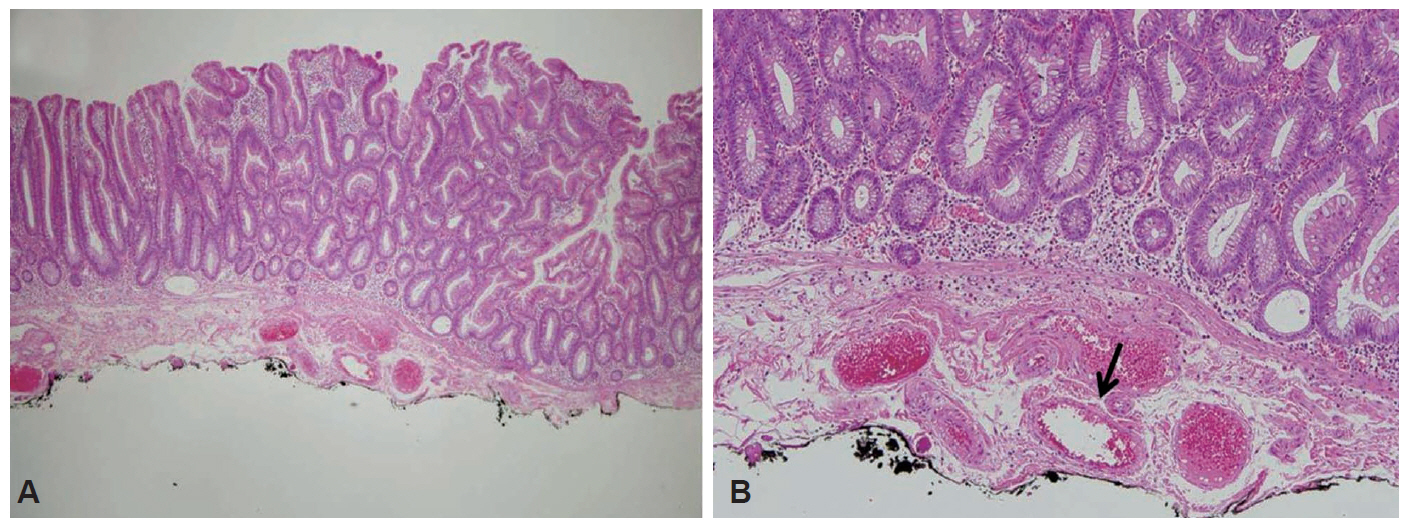
Fig. 3. Endoscopic resection specimen. (A) The specimen has mucosal and submucosal layers without the muscularis layer of the colonic wall (H&E stain, ×40). (B) Submucosal layer showing submucosal vessels (arrow) without severe coagulation damage due to thermal injury (H&E stain, ×100).

Fig. 4. Surgical resection specimen. (A) Large hematoma (long arrow) in the proper muscle layer. The endoscopic resection site (short arrows) and perforation site (arrowheads) are also shown (H&E stain, ×12.5). (B) Perforation site in the specimen (H&E stain, ×40). (C) Necrosis in the colonic wall is evident at the perforation site (arrow) (H&E stain, ×100). (D) Neutrophil infiltration is evident at the perforation site (H&E stain, ×200).
Reference
-
1. Raju GS, Saito Y, Matsuda T, Kaltenbach T, Soetikno R. Endoscopic management of colonoscopic perforations (with videos). Gastrointest Endosc. 2011; 74:1380–1388.
Article2. Panteris V, Haringsma J, Kuipers EJ. Colonoscopy perforation rate, mechanisms and outcome: from diagnostic to therapeutic colonoscopy. Endoscopy. 2009; 41:941–951.
Article3. Mizushima T, Kato M, Iwanaga I, et al. Technical difficulty according to location, and risk factors for perforation, in endoscopic submucosal dissection of colorectal tumors. Surg Endosc. 2015; 29:133–139.
Article4. Isomoto H, Nishiyama H, Yamaguchi N, et al. Clinicopathological factors associated with clinical outcomes of endoscopic submucosal dissection for colorectal epithelial neoplasms. Endoscopy. 2009; 41:679–683.
Article5. Xiao YF, Bai JY, Yu J, et al. Endoscopic treatment of delayed colon perforation: the enteroscopy overtube approach. Endoscopy. 2014; 46:503–508.
Article6. Hagel AF, Boxberger F, Dauth W, Kessler HP, Neurath MF, Raithel M. Colonoscopy-associated perforation: a 7-year survey of in-hospital frequency, treatment and outcome in a German university hospital. Colorectal Dis. 2012; 14:1121–1125.
Article7. Araghizadeh FY, Timmcke AE, Opelka FG, Hicks TC, Beck DE. Colonoscopic perforations. Dis Colon Rectum. 2001; 44:713–716.
Article8. Fujishiro M, Yahagi N, Kakushima N, et al. Outcomes of endoscopic submucosal dissection for colorectal epithelial neoplasms in 200 consecutive cases. Clin Gastroenterol Hepatol. 2007; 5:678–683.
Article9. Nakamura F, Saito Y, Sakamoto T, et al. Potential perioperative advantage of colorectal endoscopic submucosal dissection versus laparoscopy-assisted colectomy. Surg Endosc. 2015; 29:596–606.
Article10. Saito Y, Uraoka T, Yamaguchi Y, et al. A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video). Gastrointest Endosc. 2010; 72:1217–1225.
Article11. Kim ES, Cho KB, Park KS, et al. Factors predictive of perforation during endoscopic submucosal dissection for the treatment of colorectal tumors. Endoscopy. 2011; 43:573–578.
Article12. Byeon JS, Yang DH, Kim KJ, et al. Endoscopic submucosal dissection with or without snaring for colorectal neoplasms. Gastrointest Endosc. 2011; 74:1075–1083.
Article13. Lohsiriwat V. Colonoscopic perforation: incidence, risk factors, management and outcome. World J Gastroenterol. 2010; 16:425–430.
Article14. Yang DH, Byeon JS, Lee KH, et al. Is endoscopic closure with clips effective for both diagnostic and therapeutic colonoscopy-associated bowel perforation? Surg Endosc. 2010; 24:1177–1185.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Synchronous Colonic Laterally Spreading Tumors Treated by Sequential Endoscopic Submucosal Dissection Performed on Two Consecutive Days
- A Case of Pneumorrhachis and Pneumoscrotum Following Colon Endoscopic Submucosal Dissection
- Submerging Endoscopic Submucosal Dissection Leads to Successful En Bloc Resection of Colonic Laterally Spreading Tumor with Submucosal Fat
- Endoscopic Treatment Strategy for Large Laterally Spreading Tumor: Endoscopic Piecemeal Mucosal Resection or Endoscopic Submucosal Dissection
- Perforation of a Gastric Tear during Esophageal Endoscopic Submucosal Dissection under General Anesthesia
