Pediatr Gastroenterol Hepatol Nutr.
2016 Jun;19(2):143-146. 10.5223/pghn.2016.19.2.143.
Mesenteric Panniculitis in a Thirteen-Year-Old Korean Boy Treated with Prednisolone: A Case Report
- Affiliations
-
- 1Department of Pediatrics, Konkuk University School of Medicine, Seoul, Korea. baedori@hanafos.com
- 2Department of Pathology, Konkuk University School of Medicine, Seoul, Korea.
- 3Department of Radiology, Konkuk University School of Medicine, Seoul, Korea.
- 4Department of General Surgery, Konkuk University School of Medicine, Seoul, Korea.
- KMID: 2328176
- DOI: http://doi.org/10.5223/pghn.2016.19.2.143
Abstract
- Pediatric mesenteric panniculitis is an extremely rare disease of unknown etiology characterized by chronic inflammation, fat necrosis, and fibrosis in the mesenteric adipose tissue. A previously healthy 13-year-old boy was admitted because of right upper abdominal pain. An abdominal computed tomography scan revealed increased attenuation and enhancement in the left upper abdominal omental fat and anterior peritoneal wall thickening. A laparoscopic biopsy showed mesenteric panniculitis with chronic inflammation, adiponecrosis, and septal fibrosis. Serological tests for autoimmune diseases, nested polymerase chain reaction for Mycobacterium tuberculosis, and special immunohistochemical stains for malignancy were all negative. Symptomatic improvement and improved abnormal findings were achieved after an 8-month treatment with prednisolone according to a follow-up abdominal computed tomography scan. Here, we report a case of pediatric mesenteric panniculitis treated with prednisolone.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Initial abdominal computed tomography (CT) scan showed increased attenuation and enhancement of omental fat as well as anterior peritoneal wall thickening and enhancement (arrows). (B) Follow-up abdominal CT scan at 8 months showed marked improvement in intra-abdominal fat attenuation.
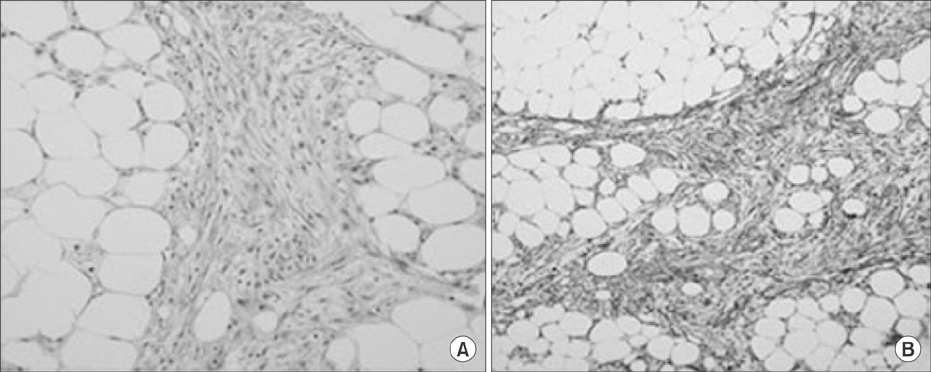
Fig. 2 Mesenteric biopsy showed nodular panniculitis, septal fibrosis with hyalinization, chronic inflammation, and fat necrosis (A: H&E, ×200; B: Masson's trichrome, ×100).
Reference
-
1. Cakmak O, Tanyel FC, Cağlar M, Göğüş S. Mesenteric panniculitis mimicking acute abdomen in a 4-year-old child. Z Kinderchir. 1986; 41:313–314.
Article2. Hakgüder G, Akgür FM, Olguner M, Ozer E, Aktug T. A case of mesenteric panniculitis in a 4-year-old child. Pediatr Int. 2000; 42:577–578.
Article3. Davis CF, Guzzetta PC, Patterson K. Primary (retractile) mesenteritis in a child. J Pediatr Surg. 1992; 27:1544–1545.
Article4. Spark RB, Yakovac WC, Wagget J. Retractile sclerosing mesenteritis. Case report. Clin Pediatr (Phila). 1971; 10:119–122.5. Viswanathan V, Murray KJ. Idiopathic sclerosing mesenteritis in paediatrics: Report of a successfully treated case and a review of literature. Pediatr Rheumatol Online J. 2010; 8:5.
Article6. Rumman N, Rumman G, Sharabati B, Zagha R, Disi N. Mesenteric panniculitis in a child misdiagnosed as appendicular mass: a case report and review of literature. Springerplus. 2014; 3:73.
Article7. Ferrari TC, Couto CM, Vilaça TS, Xavier MA, Faria LC. An unusual presentation of mesenteric panniculitis. Clinics (Sao Paulo). 2008; 63:843–844.
Article8. Ogden WW 2nd, Bradburn DM, Rives JD. Mesenteric panniculitis: review of 27 cases. Ann Surg. 1965; 161:864–875.9. Durst AL, Freund H, Rosenmann E, Birnbaum D. Mesenteric panniculitis: review of the leterature and presentation of cases. Surgery. 1977; 81:203–211.10. Horton KM, Lawler LP, Fishman EK. CT findings in sclerosing mesenteritis (panniculitis): spectrum of disease. Radiographics. 2003; 23:1561–1567.
Article11. Wat SY, Harish S, Winterbottom A, Choudhary AK, Freeman AH. The CT appearances of sclerosing mesenteritis and associated diseases. Clin Radiol. 2006; 61:652–658.
Article12. Emory TS, Monihan JM, Carr NJ, Sobin LH. Sclerosing mesenteritis, mesenteric panniculitis and mesenteric lipodystrophy: a single entity? Am J Surg Pathol. 1997; 21:392–398.
Article13. Soergel KH, Hensley GT. Fatal mesenteric panniculitis. Gastroenterology. 1966; 51:529–536.
Article14. Akram S, Pardi DS, Schaffner JA, Smyrk TC. Sclerosing mesenteritis: clinical features, treatment, and outcome in ninety-two patients. Clin Gastroenterol Hepatol. 2007; 5:589–596.
Article15. Tedeschi CG, Botta GC. Retractile mesenteritis. N Engl J Med. 1962; 266:1035–1040.
Article16. Tytgat GN, Roozendaal K, Winter W, Esseveld MR. Successful treatment of a patient with retractile mesenteritis with prednisone and azathioprine. Gastroenterology. 1980; 79:352–356.
Article17. Issa I, Baydoun H. Mesenteric panniculitis: various presentations and treatment regimens. World J Gastroenterol. 2009; 15:3827–3830.
Article18. Ginsburg PM, Ehrenpreis ED. A pilot study of thalidomide for patients with symptomatic mesenteric panniculitis. Aliment Pharmacol Ther. 2002; 16:2115–2122.
Article19. Parra-Davila E, McKenney MG, Sleeman D, Hartmann R, Rao RK, McKenney K, et al. Mesenteric panniculitis: case report and literature review. Am Surg. 1998; 64:768–771.20. Coulier B. Mesenteric panniculitis. Part 2: prevalence and natural course: MDCT prospective study. JBR-BTR. 2011; 94:241–246.
Article
