Clinical Manifestations and Outcomes of Treatment in Cytomegalovirus Endotheliitis
- Affiliations
-
- 1Department of Ophthalmology, Gyeongsang National University School of Medicine, Jinju, Korea. Maya12kim@naver.com
- 2Lee Seong Su Eye Center, Jinju, Korea.
- 3Gyeongsang Institute of Health Science, Gyeongsang National University, Jinju, Korea.
- 4Department of Laboratory Medicine, Gyeongsang National University College of Medicine, Jinju, Korea.
- KMID: 2290487
- DOI: http://doi.org/10.3341/jkos.2016.57.6.863
Abstract
- PURPOSE
To elucidate the clinical manifestations of cytomegalovirus (CMV) endotheliitis, and evaluate the outcomes of treatment in CMV endotheliitis.
METHODS
We reviewed the medical records of 7 patients (8 eyes) who were diagnosed with CMV endotheliitis via a polymerase chain reaction (PCR) of aqueous humor and were treated with ganciclovir.
RESULTS
Eight eyes of 7 patients were followed for a mean of 17.8 months. One patient had bilateral corneal endotheliitis. All eyes had coin-shaped keratoprecipitates and mild anterior chamber inflammation (1+~2+). All eyes had an absence of anterior segment inflammation 3 weeks after ganciclovir treatment. Following treatment, the mean visual acuity improved significantly from 0.60 ± 0.40 (log MAR) at baseline to 0.18 ± 0.18 (log MAR) at last follow-up. The mean intraocular pressure (IOP) decreased significantly from 30 mm Hg at baseline to 12 mm Hg at last visit. Two eyes had a recurrence of corneal endotheliitis, where one underwent penetrating keratoplasty and the other was treated with intravitreal ganciclovir injection.
CONCLUSIONS
Patients with increased IOP and coin-shaped keratoprecipitates are suspected to have CMV endotheliitis, and PCR of aqueous humor is needed to diagnose CMV endotheliitis. More than 6 weeks of ganciclovir treatment might be effective for CMV endotheliitis and may help prevent recurrence.
Keyword
MeSH Terms
Figure
-
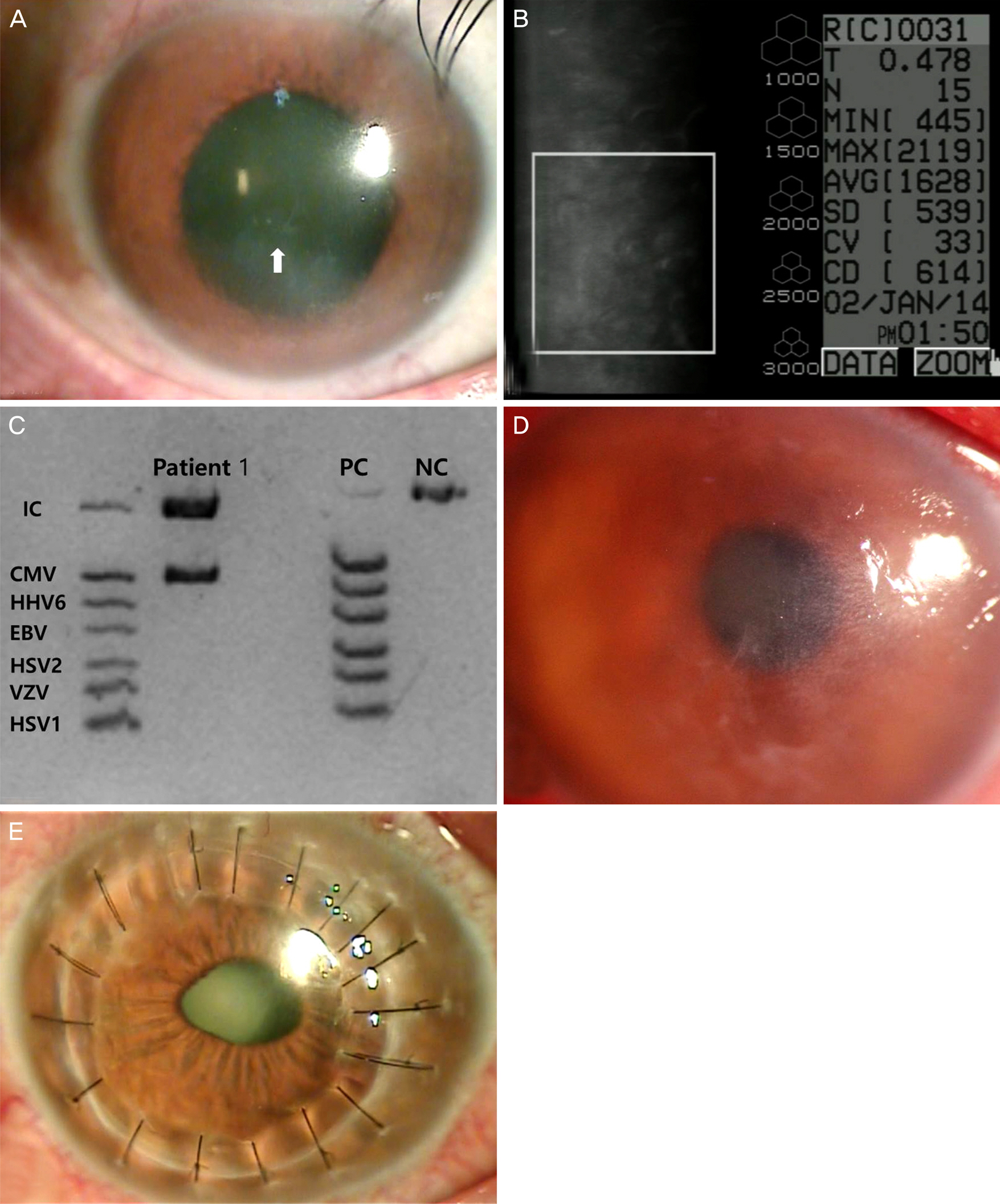
Figure 1. Clinical photographs of patient 1. Slit lamp photograph showed sectorial corneal edema and coin-shaped keratic precipitates in left eye of patient 1 (A, arrow). Specular microscopy revealed pleomorphism and polymegathism of corneal endothelial cells (B). Multiplex polymerase chain reaction showed positive in cytomegalovirus (CMV) (C). After withdrawal of valganciclovir, bullous keratopathy occurred (D). No recurrence had been occurred after penetrating keratoplasty (E). EBV = Epstein-Barr virus; HHV6 = human herpes virus 6; HSV1, 2= herpetic simplex virus 1, 2; VZV = varicella-zoster virus; IC = internal control; NC = negative control; PC = positive control.
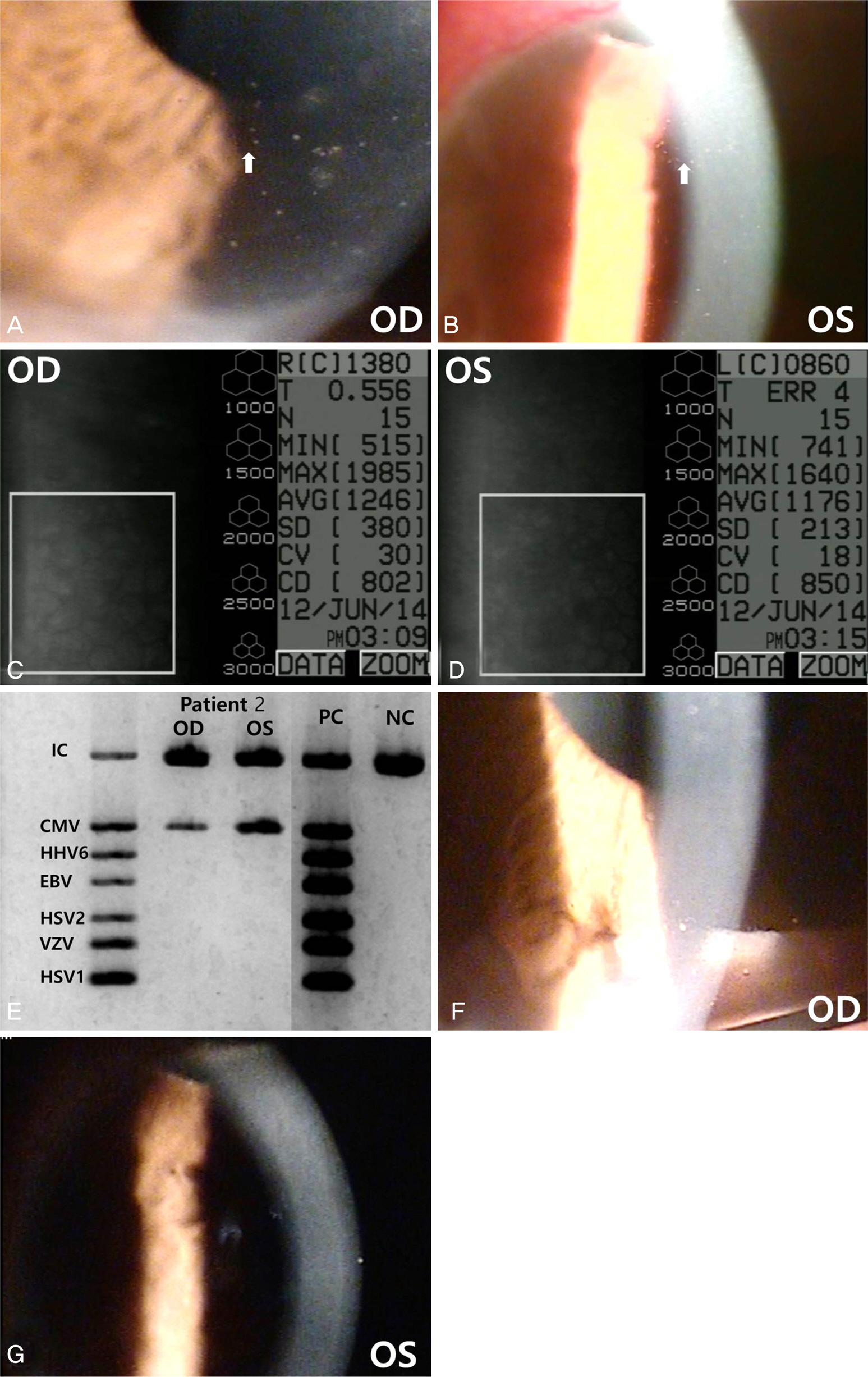
Figure 2. Clinical photographs of patient 2. Slit lamp photograph showed sectorial corneal edema and coin-shaped keratic precipitates in right eye (A, arrow) and left eye (B, arrow) of patient 2. Specular microscopy revealed decreased number, pleomorphism and polymegathism of corneal endothelial cells in right (C) and left eyes (D). Multiplex polymerase chain reaction showed positive with cytomegalovirus (CMV) in aqueous humor in both eyes (E). After valganciclovir treatment, keratic precipitates and edema of cornea were disappeared in right (F) and left eye (G). EBV = Epstein-Barr virus; HHV6 = human herpes virus 6; HSV 1, 2 = herpetic simplex virus 1, 2; VZV = Varicella-zoster virus; IC = internal control; PC = positive control; NC = negative control.
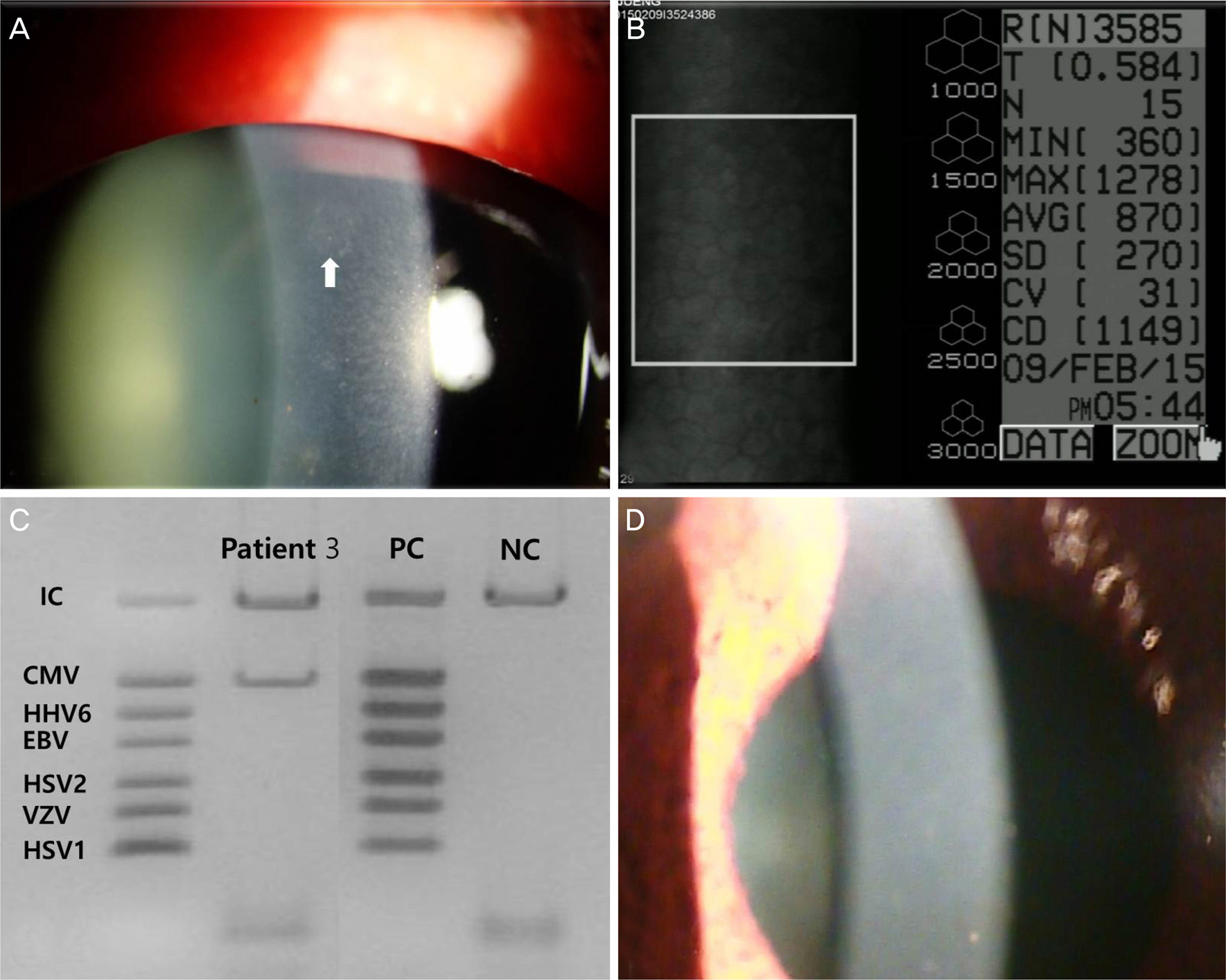
Figure 3. Clinical photographs of patient 3. Slit lamp photograph showed sectorial corneal edema and coin-shaped keratic precipitates in right eye (A, arrow) of patient 3. Specular microscopy revealed decreased number and polymegathism of corneal endothelial cells (B). Multiplex polymerase chain reaction showed positive with cytomegalovirus (CMV) in aqueous humor in right eye (C). Corneal lesions were disappeared after ganciclovir treatment (D). HHV6 = human herpes virus 6; EBV = Epstein-Barr virus; HSV1, 2 = herpetic simplex virus 1, 2; VZV = varicella-zoster virus; IC = internal control; PC = positive control; NC = negative control.
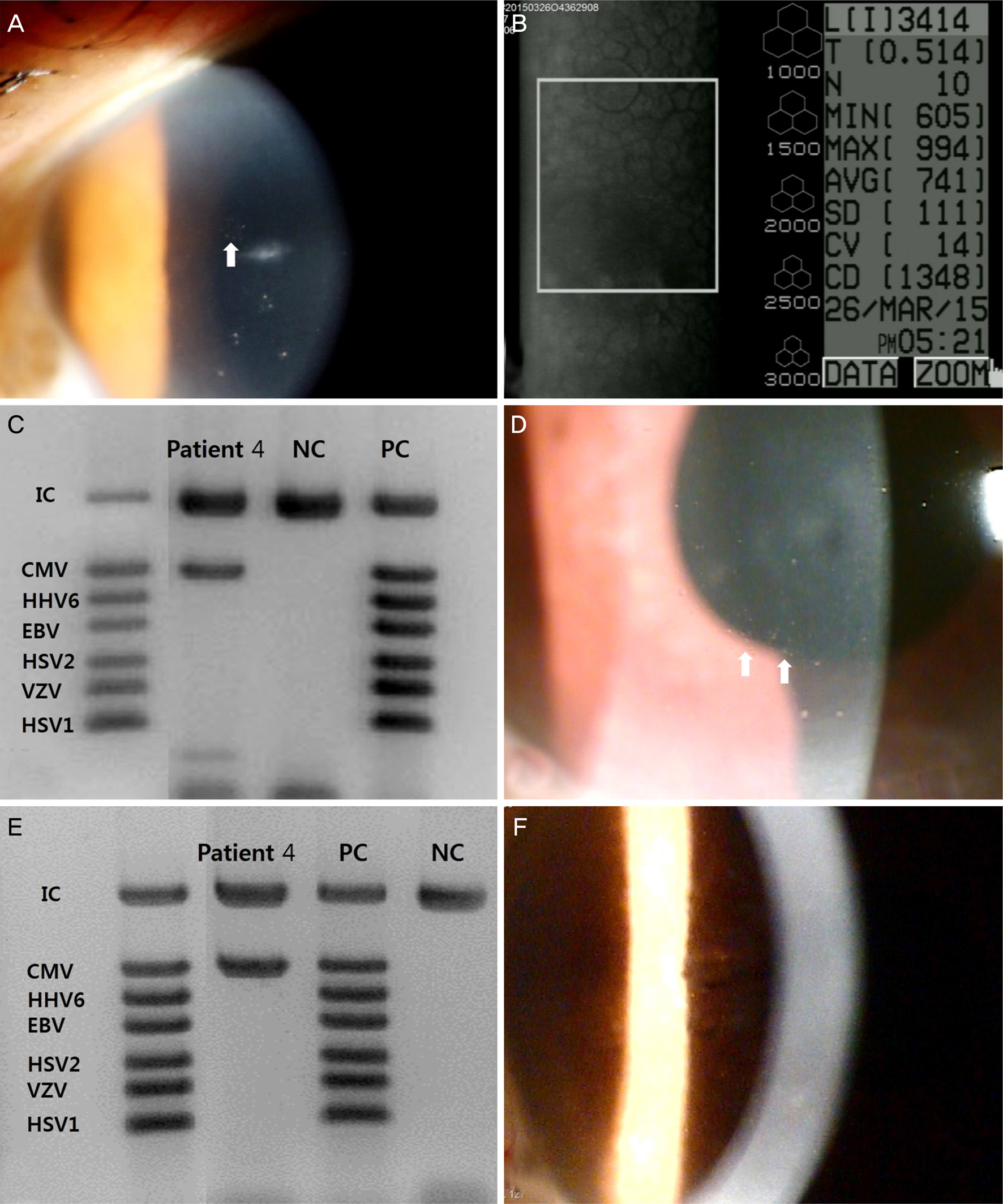
Figure 4. Clinical photographs of patient 4. Slit lamp photograph showed sectorial corneal edema and coin-shaped keratic precipitates in left eye (A, arrow) of patient 4. Specular microscopy revealed decreased number, polymegathism, pleomorphism, and hy-po-reflectivity of corneal endothelial cells (B). Multiplex polymerase chain reaction showed positive with cytomegalovirus (CMV) in aqueous humor in left eye (C). Two months after completion of ganciclovir treatment of 6 weeks, coin-shaped keratic precipitates were re-appeared in different location of cornea (D, arrows). Repeated multiplex polymerase chain reaction (PCR) revealed positive with CMV in aqueous humor (E). Corneal keratic precipitates and edema were regressed after intravitreal ganciclovir injection (F). HHV6 = human herpes virus 6; EBV = Epstein-Barr virus; HSV1, 2 = herpetic simplex virus 1, 2; VZV = Varicella-zoster virus; IC = internal control; PC = positive control; NC = negative control.

Figure 5. Clinical photographs of patient 5. Slit lamp photograph showed sectorial corneal edema and coin-shaped keratic precipitates in right eye (A, arrow) of patient 5. Specular microscopy revealed decreased number, polymegathism, and hypo-reflectivity of corneal endothelial cells (B). Multiplex polymerase chain reaction showed positive with cytomegalovirus (CMV) in aqueous humor in right eye (C). After ganciclovir treatment, coin-shaped keratic precipitate was regressed (D). HHV6 = human herpes virus 6; EBV = Epstein-Barr virus; HSV1, 2 = herpetic simplex virus 1, 2; VZV = Varicella-zoster virus; IC = internal control; PC = positive control; NC = negative control.

Figure 6. Clinical photographs of patient 6. Slit lamp photograph showed sectorial corneal edema and coin-shaped keratic precipitates in right eye at superior cornea (A, arrow) of patient 6. Specular microscopy revealed decreased number and polymegathism of corneal endothelial cells (B). Multiplex polymerase chain reaction showed positive with cytomegalovirus (CMV) in aqueous humor in right eye (C). Corneal lesions were disappeared after ganciclovir treatment (D). HHV6 = human herpes virus 6; EBV = Epstein-Barr virus; HSV1, 2 = herpetic simplex virus 1, 2; VZV = Varicella-zoster virus; IC = internal control; PC = positive control; NC = negative control.

Figure 7. Clinical photographs of patinet 7. Slit lamp photograph showed sectorial corneal edema and coin-shaped keratic precipitates in left eye at inferior cornea (A, black and white arrow) of patient 7. Specular microscopy revealed decreased number of corneal endothelial cells (B). Multiplex polymerase chain reaction showed positive with cytomegalovirus (CMV) in aqueous humor in left eye (C). After ganciclovir treatment, lesions of cornea were vanished (D). HHV6 = human herpes virus 6; EBV = Epstein-Barr virus; HSV1, 2 = herpetic simplex virus 1, 2; VZV = Varicella-zoster virus; IC = internal control; PC = positive control; NC = negative control.
Cited by 1 articles
-
Epstein-Barr Virus-related Corneal Endotheliitis Accompanied with Secondary Glaucoma
Yong Wun Cho, Hyun Ji Kang, Gyu Nam Kim, Hyun A Kim, In Young Chung, Seong Jae Kim
J Korean Ophthalmol Soc. 2020;61(2):205-208. doi: 10.3341/jkos.2020.61.2.205.
Reference
-
References
1. Suzuki T, Ohashi Y. Corneal endotheliitis. Semin Ophthalmol. 2008; 23:235–40.
Article2. Koizumi N, Yamasaki K, Kawasaki S, et al. Cytomegalovirus in aqueous humor from an eye with corneal endotheliitis. Am J Ophthalmol. 2006; 141:564–5.
Article3. Koizumi N, Suzuki T, Uno T, et al. Cytomegalovirus as an etiologic factor in corneal endotheliitis. Ophthalmology. 2008; 115:292–7.e3.
Article4. Koizumi N, Inatomi T, Suzuki T, et al. Clinical features and abdominal of cytomegalovirus corneal endotheliitis: analysis of 106 cases from the Japan corneal endotheliitis study. Br J Ophthalmol. 2015; 99:54–8.5. Choi WS, Cho JH, Kim HK, et al. A case of CMV endotheliitis treated with intravitreal ganciclovir injection. Korean J Ophthalmol. 2013; 27:130–2.
Article6. Shin SY, Kwon KC, Park JW, et al. Evaluation of the Seeplex(R) Meningitis ACE Detection kit for the detection of 12 common abdominal and viral pathogens of acute meningitis. Ann Lab Med. 2012; 32:44–9.7. Hwang YS, Shen CR, Chang SH, et al. The validity of clinical abdominal profiles for cytomegaloviral anterior segment infection. Graefes Arch Clin Exp Ophthalmol. 2011; 249:103–10.8. Chee SP, Jap A. Treatment outcome and risk factors for visual loss in Cytomegalovirus endotheliitis. Graefes Arch Clin Exp Ophthalmol. 2012; 250:383–9.
Article9. Chee SP, Bascal K, Jap A, et al. Clinical features of cytomeglovirus anterior uveitis in immunocompetent patients. Am J Ophthalmol. 2008; 145:834–40.10. Anshu A, Chee SP, Mehta JS, Tan DT. Cytomegalovirus endotheliitis in Descemet's stripping endothelial keratoplasty. Ophthalmology. 2009; 116:624–30.
Article11. Alfawaz A. Cytomegalovirus-related corneal endotheliitis: a abdominal article. Saudi J Ophthalmol. 2013; 27:47–9.12. Su CC, Wang IJ, Chen WL, et al. Topical ganciclovir treatment in patients with cytomegalovirus endotheliitis receiving penetrating keratoplasty. Clin Experiment Ophthalmol. 2013; 41:339–47.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Atypical Cytomegalovirus Corneal Endotheliitis after Intravitreal Triamcinolone Injection
- A Case of Cytomegalovirus Corneal Endotheliitis Almost Misdiagnosed as Corneal Graft Rejection
- Analysis of Clinical Manifestations and Prognostic Factors in Herpetic Endotheliitis
- Clinical Manifestations and Outcomes of Varicella-zoster Virus Endotheliitis
- A Case of CMV Endotheliitis Treated with Intravitreal Ganciclovir Injection
