Recurrent Streptococcus Pneumoniae Meningoencephalitis in a Patient With a Transethmoidal eningoencephalocele
- Affiliations
-
- 1Department of Neurology, Chonbuk National University Medical School and Hospital, Jeonju, Korea. jeongsk@chonbuk.ac.kr
- KMID: 2287685
- DOI: http://doi.org/10.3988/jcn.2008.4.1.40
Abstract
- We report a case of recurrent Streptococcus Pneumoniae meningoencephalitis with a transethmoidal meningoencephalocele (TEME) but without cerebrospinal fluid (CSF) leakage. A 35-year-old man was admitted with S. pneumoniae meningitis. He had suffered from four episodes of recurrent pneumococcal meningitis during the previous 4 years. A computed tomography scan of the paranasal sinus showed the TEME protruding through a bony defect of the right frontal base. However, the patient did not have symptoms that could be attributable to CSF leakage, and radioisotope cisternography did not identify a leak. Brain magnetic resonance imaging revealed cortical lesions overlying the TEME, and electroencephalography revealed epileptiform discharges in frontal regions. Appropriate antibiotics therapy without steroids was given to improve his condition. The presented case suggests that even in the absence of clinically demonstrable CSF leakage, an occult skullbase defect and its associated meningoencephalocele should be considered in patients with recurrent bacterial meningitis.
MeSH Terms
Figure
-

Figure 1 Coronal (A) and sagittal (B) computed tomography views of the paranasal sinus, showing a bony defect of the right frontal base and a cystic mass lesion protruding into the ethmoid sinus (arrow).

Figure 2 Radioisotope cisternography, indicating CSF activity with no leakage at the right frontal base in the 4-hour-delayed image (arrow). RL: Right lateral view.

Figure 3 Brain magnetic resonance images. (A) Coronal FLAIR image, showing cerebral tissue herniating into the right ethmoid sinus and a focal encephalomalatic change in the anteroinferior aspect of the right frontal lobe (arrow). (B) Diffusion-weighted image showing the left lateral ventricle filled with small amounts of irregular debris, indicating pyogenic ventriculitis (arrow).
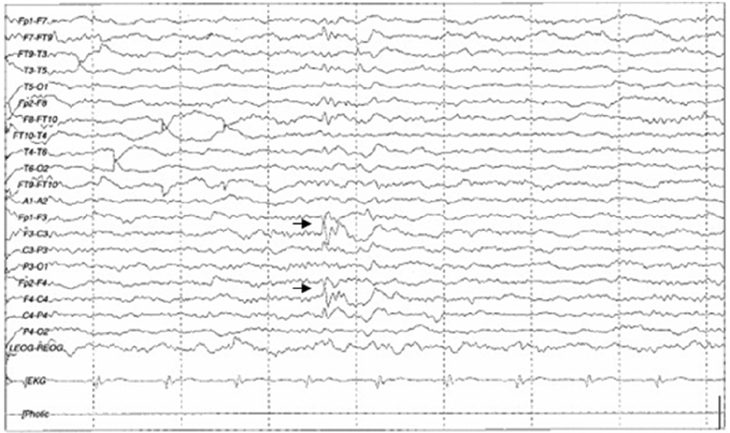
Figure 4 Electroencephalogram showing spike-and-slow wave complexes with phase reversal in frontal regions (arrow).
Reference
-
1. Gilbert B, Menetrey C, Belin V, Brosset P, de Lumley L, Fisher A. Familial isolated congenital asplenia: a rare, frequently hereditary dominant condition, often detected too late as a cause of overwhelming pneumococcal sepsis. Report of a new case and review of 31 others. Eur J Pediatr. 2002. 161:368–372.
Article2. Heckmann JG, Schüttler M, Dörfler A. Pneumococcal meningoencephalitis. Wien Klin Wochenschr. 2005. 117:739.
Article3. Morand PC, Veuillez V, Poyart C, Abachin E, Quesne G, Dupont B, et al. Recurrent pneumococcal meningitis in a splenectomised HIV-infected patient. Ann Clin Microbiol Antimicrob. 2003. 2:9.4. Drummond DS, de Jong AL, Giannoni C, Sulek M, Friedman EM. Recurrent meningitis in the pediatric patient - the otolaryngologist's role. Int J Pediatr Otorhinolaryngol. 1999. 48:199–208.
Article5. Kendirli T, Ünay B, Tosun F, Hacihamdioğlu B, Akin R, Özkaptan Y, et al. Recurrent Streptococcus pneumoniae meningitis in a child with traumatic anterior cranial base defect. Pediatr Int. 2006. 48:91–93.
Article6. Rupa V, Rajshekhar V, Weider DJ. Syndrome of recurrent meningitis due to congenital perilymph fistula with two different clinical presentations. Int J Pediatr Otorhinolaryngol. 2000. 54:173–177.
Article7. Dempsey PK, Harbaugh RE. Encephalomeningocele presenting with spontaneous cerebrospinal fluid rhinorrhea in an elderly man: case report. Neurosurgery. 1988. 23:637–640.
Article8. Davachi F, Bregu H, Lito G. Recurrent Streptococcus pneumoniae meningitis. J Trop Pediatr. 2002. 48:249–251.
Article9. Hur HY, Ahn GH, Chae KY. A case of spontaneous transsphenoidal encephalocele with recurrent bacterial meningitis. J Korean Child Neurol Soc. 2007. 15:116–120.10. Jorens PG, Parizel PM, Demey HE, Smets K, Jadoul K, Verbeek MM, et al. Meningoencephalitis caused by Streptococcus pneumoniae: a diagnostic and therapeutic challenge. Diagnosis with diffusion-weighted MRI leading to treatment with corticosteroids. Neuroradiology. 2005. 47:758–764.
Article11. Pollock JA, Newton TH, Hoyt WF. Transsphenoidal and transethmoidal encephaloceles. A review of clinical and roentgen features in 8 cases. Radiology. 1968. 90:442–453.12. Garg P, Rathi V, Bhargava SK, Aggarwal A. CSF rhinorrhea and recurrent meningitis caused by transethmoidal meningoencephaloceles. Indian Pediatr. 2005. 42:1033–1036.13. Hasegawa T, Sugeno N, Shiga Y, Takeda A, Karibe H, Tominaga T, et al. Transethmoidal intranasal meningoencephalocele in an adult with recurrent meningitis. J Clin Neurosci. 2005. 12:702–704.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of meningoencephalitis due to streptococcus pneumoniae in a patients with chronic graft-versus-host disease after allogeneic bone marrow transplantation
- Antibiotic-Resistant Streptococcus pneumoniae
- A case of fatal pneumococcal 19A meningoencephalitis despite administration of seven-valent pneumococcal conjugate vaccines
- Serial Magnetic Resonance Imagings of Multiple Brain Abscesses in a Patient with Pneumococcal Meningoencephalitis
- Penicillin-resistant Streptococcus pneumoniae
