Transesophageal Echocardiographic Findings Are Independent and Relevant Predictors of Ischemic Stroke in Patients with Nonvalvular Atrial Fibrillation
- Affiliations
-
- 1Department of Neurology, Toyama University Hospital, Toyama, Japan. shutaro@med.u-toyama.ac.jp
- 2Second Department of Internal Medicine, Toyama University Hospital, Toyama, Japan.
- KMID: 2287587
- DOI: http://doi.org/10.3988/jcn.2012.8.3.170
Abstract
- BACKGROUND AND PURPOSE
Not only clinical factors, including the CHADS2 score, but also echocardiographic findings have been reported to be useful for predicting the risk of ischemic stroke in patients with nonvalvular atrial fibrillation (NVAF). However, it remains to be determined which of these factors might be more relevant for evaluation of the risk of stroke in each patient.
METHODS
In 490 patients with NVAF who underwent transesophageal echocardiography (TEE), we examined the long-term incidence of ischemic stroke events (mean follow-up time, 5.7+/-3.3 years). For each patient, the predictive values of gender, the CHADS2 risk factors (congestive heart failure, hypertension, age > or =75 years, diabetes mellitus, history of cerebral ischemia), the CHADS2 score, and the findings on echocardiography, including TEE risk markers, were assessed.
RESULTS
The ischemic stroke rate was significantly correlated with the CHADS2 score (p<0.05). According to the results of univariate analyses, age > or =75 years, history of cerebral ischemia, CHADS2 score > or =2, and presence of TEE risk were significantly correlated with the incidence of ischemic stroke. Cox proportional hazards regression analyses identified age > or =75 years and presence of TEE risk as significant predictors of subsequent ischemic stroke events in patients with NVAF. As compared with that in persons below 75 years of age without TEE risk, the ischemic stroke rate was significantly higher in persons who were > or =75 years of age with TEE risk (4.3 vs. 0.56%/year, adjusted hazard ratio=8.94, p<0.001).
CONCLUSIONS
TEE findings might be more relevant predictors of ischemic stroke than the CHADS2 score in patients with NVAF. The stroke risk was more than 8-fold higher in patients aged > or =75 years with TEE risk.
MeSH Terms
Figure
-
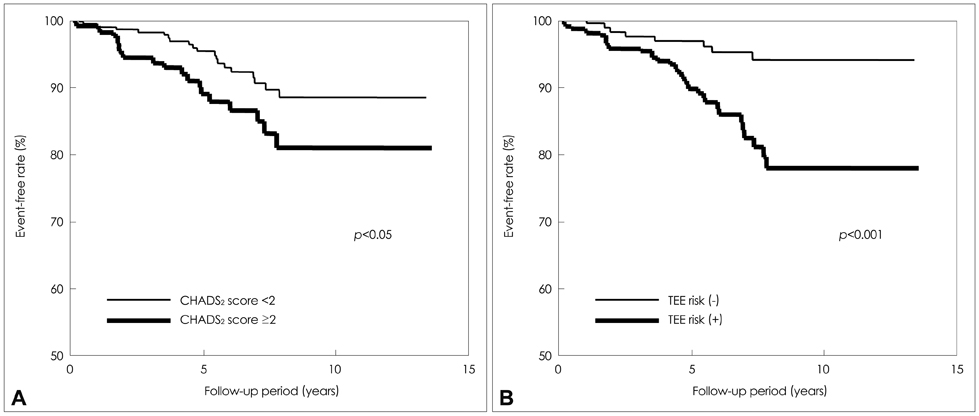
Fig. 1 A: Kaplan-Meier survival curves for ischemic stroke by the CHADS2 score in patients with NVAF. The incidence of ischemic stroke in patients with a CHADS2 score of less than 2 was 1.18% per year, while that in patients with a CHADS2 score of 2 or over was 2.19% per year (log-rank test, p<0.05). B: Kaplan-Meier survival curves for ischemic stroke according to the presence/absence of TEE risk in patients with NVAF. The incidence of ischemic stroke in patients without TEE risk was 0.67% per year, while that in patients with TEE risk was 2.26% per year (log-rank test, p<0.001). NVAF: nonvalvular atrial fibrillation, TEE: transesophageal echocardiography.

Fig. 2 Kaplan-Meier survival curves for ischemic stroke using the combination of age and TEE risk in patients with NVAF. The incidence of ischemic stroke was 0.56% per year in patients younger than 75 years of age without TEE risk, but 4.3% per year in patients aged 75 years or older with TEE risk (log-rank test, p<0.001). NVAF: nonvalvular atrial fibrillation, TEE: transesophageal echocardiography.
Cited by 1 articles
-
Spontaneous Conversion of Atrial Fibrillation to Normal Sinus Rhythm Following Recurrent Cerebral Infarctions
Kyungmi Oh, Jeong-Yoon Choi, Byung-Jo Kim
J Korean Neurosurg Soc. 2013;53(6):368-370. doi: 10.3340/jkns.2013.53.6.368.
Reference
-
1. Yokota C, Minematsu K, Hasegawa Y, Yamaguchi T. Long-term prognosis, by stroke subtypes, after a first-ever stroke: a hospital-based study over a 20-year period. Cerebrovasc Dis. 2004. 18:111–116.
Article2. Marini C, De Santis F, Sacco S, Russo T, Olivieri L, Totaro R, et al. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: results from a population-based study. Stroke. 2005. 36:1115–1119.
Article3. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991. 22:983–988.
Article4. Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001. 285:2370–2375.
Article5. Stroke Prevention in Atrial Fibrillation Investigators Committee on Echocardiography. Transesophageal echocardiographic correlates of thromboembolism in high-risk patients with nonvalvular atrial fibrillation. Ann Intern Med. 1998. 128:639–647.6. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001. 285:2864–2870.
Article7. Fatkin D, Kelly RP, Feneley MP. Relations between left atrial appendage blood flow velocity, spontaneous echocardiographic contrast and thromboembolic risk in vivo. J Am Coll Cardiol. 1994. 23:961–969.
Article8. Stroke Prevention in Atrial Fibrillation Investigators Committee on Echocardiography. Transesophageal echocardiography in atrial fibrillation: standards for acquisition and interpretation and assessment of interobserver variability. J Am Soc Echocardiogr. 1996. 9:556–566.9. Weir NU. An update on cardioembolic stroke. Postgrad Med J. 2008. 84:133–142.
Article10. Stroke Risk in Atrial Fibrillation Working Group. Comparison of 12 risk stratification schemes to predict stroke in patients with nonvalvular atrial fibrillation. Stroke. 2008. 39:1901–1910.11. Hart RG, Pearce LA. Current status of stroke risk stratification in patients with atrial fibrillation. Stroke. 2009. 40:2607–2610.
Article12. Kleemann T, Becker T, Strauss M, Schneider S, Seidl K. Prevalence and clinical impact of left atrial thrombus and dense spontaneous echo contrast in patients with atrial fibrillation and low CHADS2 score. Eur J Echocardiogr. 2009. 10:383–388.
Article13. Ohara K, Hirai T, Fukuda N, Sakurai K, Nakagawa K, Nozawa T, et al. Relation of left atrial blood stasis to clinical risk factors in atrial fibrillation. Int J Cardiol. 2009. 132:210–215.
Article14. Wysokinski WE, Ammash N, Sobande F, Kalsi H, Hodge D, McBane RD. Predicting left atrial thrombi in atrial fibrillation. Am Heart J. 2010. 159:665–671.
Article15. Nakagawa K, Hirai T, Sakurai K, Ohara K, Nozawa T, Inoue H. Thoracic aortic plaque enhances hypercoagulability in patients with nonrheumatic atrial fibrillation. Circ J. 2007. 71:52–56.
Article16. European Heart Rhythm Association. European Association for Cardio-Thoracic Surgery. Camm AJ, Kirchhof P, Lip GY, Schotten U, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010. 31:2369–2429.17. Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011. 123:e269–e367.18. Nozawa T, Inoue H, Hirai T, Iwasa A, Okumura K, Lee JD, et al. D-dimer level influences thromboembolic events in patients with atrial fibrillation. Int J Cardiol. 2006. 109:59–65.
Article19. Dougu N, Takashima S, Sasahara E, Taguchi Y, Toyoda S, Hirai T, et al. Differential diagnosis of cerebral infarction using an algorithm combining atrial fibrillation and D-dimer level. Eur J Neurol. 2008. 15:295–300.
Article20. Yamaguchi T. Japanese Nonvalvular Atrial Fibrillation-Embolism Secondary Prevention Cooperative Study Group. Optimal intensity of warfarin therapy for secondary prevention of stroke in patients with nonvalvular atrial fibrillation : a multicenter, prospective, randomized trial. Stroke. 2000. 31:817–821.
Article21. Shen AY, Yao JF, Brar SS, Jorgensen MB, Chen W. Racial/ethnic differences in the risk of intracranial hemorrhage among patients with atrial fibrillation. J Am Coll Cardiol. 2007. 50:309–315.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Comparative Study on Cerebral Infarction in Patient with Nonvalvular and Valvular Atrial Fibrillation
- The Mechanism of and Preventive Therapy for Stroke in Patients with Atrial Fibrillation
- Application of New Oral Anticoagulants: Prevention of Stroke in Patients with Nonvalvular Atrial Fibrillation
- Impact of Left Atrial or Left Atrial Appendage Thrombus on Stroke Outcome: A Matched Control Analysis
- Relation of Stroke Risk Factors to Severity and Disability after Ischemic Stroke
