Atrial Mechanical Function After Maze Procedure for Atrial Fibrillation Concomitant With Mitral Valve Surgery
- Affiliations
-
- 1Division of Cardiology, Cardiac and Vascular Center, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. yk.on@samsung.com
- 2Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2225709
- DOI: http://doi.org/10.4070/kcj.2008.38.11.606
Abstract
- BACKGROUND AND OBJECTIVES
The maze procedure is effective in restoring sinus rhythm (SR) in patients with atrial fibrillation (AF). We compared the left atrial mechanical function (LAMF) of patients whose rhythm was converted to SR after maze procedure with that of patients whose rhythm was not converted to SR and determined if preoperative left atrial volume index (LAVI) and immediate postoperative LAMF could predict conversion of AF to SR. SUBJECTS AND METHODS: We prospectively evaluated 80 patients with AF treated with the maze procedure between March 2005 and February 2007. LAMF was assessed by looking at left atrial ejection volume (LAEV) and ejection fraction (LAEF) during echocardiography before, 2 weeks after, and 6 months after the procedure. RESULTS: Of the 80 enrolled patients, 71 were converted to SR after the maze procedure (SR group), and 9 were not converted to SR (AF group). There were no significant differences in age, sex, hypertension, diabetes mellitus, renal failure, stroke, thyroid dysfunction, or smoking history between the groups. Pre-operative LAVI (p=0.010) was a predictor of conversion of AF to SR. LAEF gradually increased in the SR group during follow-up, but not in the AF group. CONCLUSION: LAMF recovered in the SR group after the maze procedure, irrespective of clinical presentation and initial LAMF. Preoperative LAVI predicted SR conversion.
MeSH Terms
Figure
-
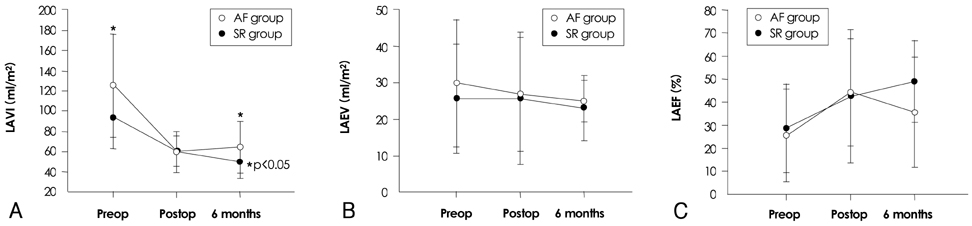
Fig. 1 Changes in LAVI, LAEV, and LAEF in the AF and SR groups. A: changes in LAVI in the AF and SR groups. The LAVI decreased gradually during the follow-up period in the SR group. In the AF group, LAVI decreased in the immediate postoperative period, but thereafter, LAVI returned to the preoperative level during the follow-up period. B: changes in LAEV in the AF and SR groups. The SR group exhibited no significant changes in LAEV between the pre- and post-operative states, whereas the AF group exhibited a gradual decrease in LAEV during the follow-up period. C: changes in LAEF in the AF and SR groups. In the AF group, the LAEF increased in the immediate postoperative period, but thereafter it returned to the preoperative level during the follow-up period. The SR group showed a gradual increase in LAEF during the follow-up period. LAVI: left atrial volume index, LAEV: left atrial ejection volume, LAEF: left atrial ejection fraction, AF: atrial fibrillation, SR: sinus rhythm, Preop: before the maze procedure, Postop: immediately (<2 weeks) after the maze procedure, 6 months: 6 months after the maze procedure.

Fig. 2 The area under the receiver operating characteristic (ROC) curve for LAVI before the maze procedure. The ROC curve for LAVI levels was 0.73 (p=0.03, 95% confidence interval 0.519-0.923), and the most reliable LAVI cut-off level to differentiate the SR group from the AF group was 117.7 mL/m2. LAVI: left atrial volume index, AF: atrial fibrillation, SR: sinus rhythm.
Cited by 1 articles
-
Characteristics of P wave in Patients with Sinus Rhythm after Maze Operation
Hyo Eun Park, Kyung-Hwan Kim, Ki-Bong Kim, Hyuk Ahn, Yun-Shik Choi, Seil Oh
J Korean Med Sci. 2010;25(5):712-715. doi: 10.3346/jkms.2010.25.5.712.
Reference
-
1. Cox JL, Boineau JP, Schuessler RB, Kater KM, Lappas DG. Five-year experience with the maze procedure for atrial fibrillation. Ann Thorac Surg. 1993. 56:814–823. discussion 823-4.2. Cox JL, Boineau JP, Schuessler RB, et al. Successful surgical treatment of atrial fibrillation: review and clinical update. JAMA. 1991. 266:1976–1980.3. Cox JL, Schuessler RB, D'Agostino HJ Jr, et al. The surgical treatment of atrial fibrillation: III. development of a definitive surgical procedure. J Thorac Cardiovasc Surg. 1991. 101:569–583.4. Cox JL, Canavan TE, Schuessler RB, et al. The surgical treatment of atrial fibrillation: II. intraoperative electrophysiologic mapping and description of the electrophysiologic basis of atrial flutter and atrial fibrillation. J Thorac Cardiovasc Surg. 1991. 101:406–426.5. Cox JL, Schuessler RB, Boineau JP. The surgical treatment of atrial fibrillation: I. summary of the current concepts of the mechanisms of atrial flutter and atrial fibrillation. J Thorac Cardiovasc Surg. 1991. 101:402–405.6. Kosakai Y, Kawaguchi AT, Isobe F, et al. Cox maze procedure for chronic atrial fibrillation associated with mitral valve disease. J Thorac Cardiovasc Surg. 1994. 108:1049–1054. discussion 1054-5.7. Kawaguchi AT, Kosakai Y, Sasako Y, Eishi K, Nakano K, Kawashima Y. Risks and benefits of combined maze procedure for atrial fibrillation associated with organic heart disease. J Am Coll Cardiol. 1996. 28:985–990.8. Yuda S, Nakatani S, Isobe F, Kosakai Y, Miyatake K. Comparative efficacy of the maze procedure for restoration of atrial contraction in patients with and without giant left atrium associated with mitral valve disease. J Am Coll Cardiol. 1998. 31:1097–1102.9. Feinberg MS, Waggoner AD, Kater KM, Cox JL, Lindsay BD, Perez JE. Restoration of atrial function after the maze procedure for patients with atrial fibrillation: assessment by Doppler echocardiography. Circulation. 1994. 90:II285–II292.10. Giardina EG. Atrial fibrillation and stroke: elucidating a newly discovered risk factor. Am J Cardiol. 1997. 80:11D–8D. discussion 35D-9D.11. Cox JL, Ad N, Palazzo T. Impact of the maze procedure on the stroke rate in patients with atrial fibrillation. J Thorac Cardiovasc Surg. 1999. 118:833–840.12. Sandoval N, Velasco VM, Orjuela H, et al. Concomitant mitral valve or atrial septal defect surgery and the modified Cox-maze procedure. Am J Cardiol. 1996. 77:591–596.13. Izumoto H, Kawazoe K, Kitahara H, et al. Can the maze procedure be combined safely with mitral valve repair? J Heart Valve Dis. 1997. 6:166–170.14. Itoh T, Okamoto H, Nimi T, et al. Left atrial function after Cox's maze operation concomitant with mitral valve operation. Ann Thorac Surg. 1995. 60:354–359. discussion 359-60.15. Yashima N, Nasu M, Kawazoe K, Hiramori K. Serial evaluation of atrial function by Doppler echocardiography after the maze procedure for chronic atrial fibrillation. Eur Heart J. 1997. 18:496–502.16. Kobayashi J, Yamamoto F, Nakano K, Sasako Y, Kitamura S, Kosakai Y. Maze procedure for atrial fibrillation associated with atrial septal defect. Circulation. 1998. 98:19 Suppl. II399–II402.17. Yuda S, Nakatani S, Kosakai Y, Yamagishi M, Miyatake K. Long-term follow-up of atrial contraction after the maze procedure in patients with mitral valve disease. J Am Coll Cardiol. 2001. 37:1622–1627.18. Kim YJ, Sohn DW, Park DG, et al. Restoration of atrial mechanical function after maze operation in patients with structural heart disease. Am Heart J. 1998. 136:1070–1074.19. Scherer M, Therapidis P, Miskovic A, Moritz A. Left atrial size reduction improves the sinus rhythm conversion rate after radiofrequency ablation for continuous atrial fibrillation in patients undergoing concomitant cardiac surgery. Thorac Cardiovasc Surg. 2006. 54:34–38.20. Chen MC, Chang JP, Guo GB, Chang HW. Atrial size reduction as a predictor of the success of radiofrequency maze procedure for chronic atrial fibrillation in patients undergoing concomitant valvular surgery. J Cardiovasc Electrophysiol. 2001. 12:867–874.21. Kim YH, Lee SC, Oh HS, et al. Predictors of sinus rhythm restoration after maze operation and relationship between pre- and post-operative left atrial volume. Korean Circ J. 2004. 34:610–614.22. Chen MC, Chang JP, Chang HW, et al. Clinical determinants of sinus conversion by radiofrequency maze procedure for persistent atrial fibrillation in patients undergoing concomitant mitral valvular surgery. Am J Cardiol. 2005. 96:1553–1557.23. Gillinov AM, Sirak J, Blackstone EH, et al. The Cox maze procedure in mitral valve disease: predictors of recurrent atrial fibrillation. J Thorac Cardiovasc Surg. 2005. 130:1653–1660.24. Seo JD, Kim CH, Oh BH, Park YB, Choi YS, Lee YW. Relation between atrial fibrillation and echocardiographic size of left atrium. Korean Circ J. 1987. 17:615–620.25. Chen MC, Chang JP, Chang HW. Preoperative atrial size predicts the success of radiofrequency maze procedure for permanent atrial fibrillation in patients undergoing concomitant valvular surgery. Chest. 2004. 125:2129–2134.26. Kim YJ, Sohn DW, Choe SJ, et al. Restoration of atrial mechanical function after maze opeartion. Korean Circ J. 1996. 26:1137–1143.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Cox-Maze Procedure for Atrial Fibrillation not Associated with Mitral Valve Disease: Report of three cases
- Mid-term Result of Operations for Atrial Fibrillation
- Change of the Left Atrial Dimension and Transport Function after the Cox-Maze Procedure for Treating Atrial Fibrillation Associated with Mitral Valve Disease: the Short-term and Mid-Term Results
- Outcome of Concomitant Cox Maze Procedure with Narrow Mazes and Left Atrial Volume Reduction
- The Clinical Outcome of Maze Procedure in Atrial Functional Mitral Regurgitation
