Heart Rate Acceleration of a Subsidiary Pacemaker by beta-Adrenergic Stimulation
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. cby6908@yuhs.ac
- 2Division of Cardiology, Department of Internal Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- KMID: 2225074
- DOI: http://doi.org/10.4070/kcj.2011.41.11.658
Abstract
- BACKGROUND AND OBJECTIVES
Recent evidence indicates that the membrane voltage and Ca2+ clocks jointly regulate sinoatrial node (SAN) automaticity. However, the mechanism of heart rhythm acceleration of the subsidiary pacemaker (SP) during beta-adrenergic stimulation is still unknown. Here we tested the hypothesis that the heart rate acceleration of the SP by beta-adrenergic stimulation involves synergistic interactions between both clock mechanisms.
SUBJECTS AND METHODS
We performed optical mapping and pharmacological interventions in 15 isolated Langendorff-perfused canine right atriums (RA). The SP model was produced by ligation of the SAN artery at the mid portion of the sulcus terminalis.
RESULTS
In the 6 RAs with an intact SAN, 1 micromol/L isoproterenol infusion increased the heart rate from 82+/-9 to 166+/-18 bpm (102%) with late diastolic Cai elevation (LDCAE) at the superior SAN. However, in the 6 SP models, the heart rate increased from 55+/-10 bpm to 106+/-11 bpm (92%, p=0.005) without LDCAE at the earliest activation site. The isoproterenol induced heart rate increase was reversed to 74+/-5 bpm (33% from baseline) by administering an infusion of the funny current blocker ZD 7288 (3 micromol/L, n=3), whereas, it was suppressed to 69+/-7 bpm (24% from baseline) by sarcoplasmic reticulum (SR) Ca2+ emptying with administering ryanodine (10 micromol/L) plus thapsigargin (200 nmol/L, n=3). The isoproterenol induced heart rate increase was completely abolished by combined treatment with funny current blocker and SR Ca2+ emptying (n=3).
CONCLUSION
Acceleration of the Ca2+ clock in the SP plays an important role in the heart rate acceleration during beta-adrenergic stimulation, and this interacts synergistically with the voltage clock to increase the heart rate.
MeSH Terms
Figure
-
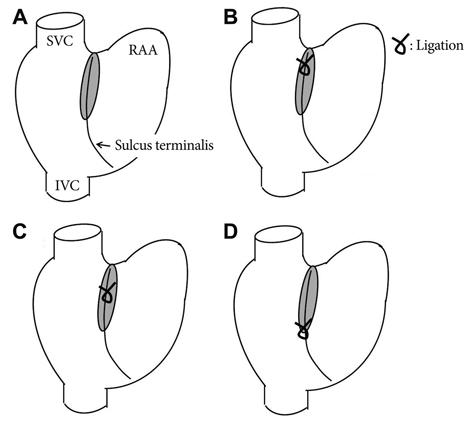
Fig. 1 The various pacemaker models. A: intact RA and superior SAN model. B: middle SAN model. C: inferior SAN model. D: subsidiary pacemaker model. The subsidiary pacemaker model was produced by the ligation of the SAN artery. SAN: sinoatrial node, RA: right atrium, SVC: superior rena cava, IVC: inferior vena cava, RAA: right atrium appendage.
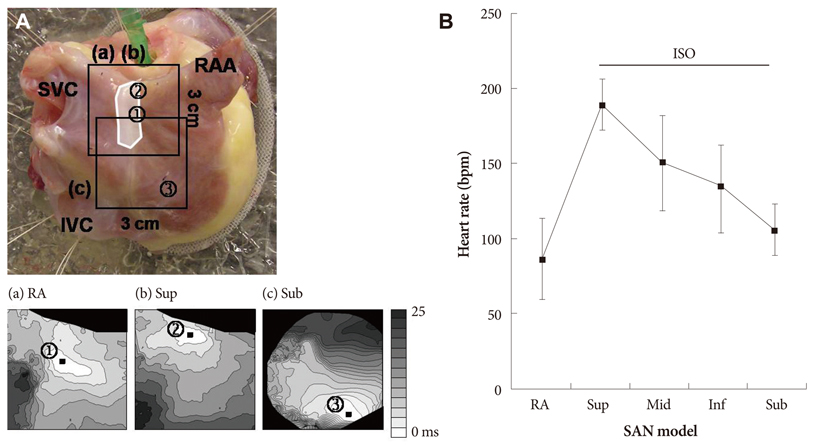
Fig. 2 The effects of sequential ligation of the SAN artery on the heart rate and the leading pacemaking sites. A, Upper panel: epicardial photographs of a perfused right atrial preparation with 3×3 cm optical fields of view. The upper and lower boxes present the optical fields of Fig. a-b and c, respectively. Lower panels: Vm isochronal maps of the RA (a), the superior SAN (b) and the subsidiary pacemaker model (c). B: heart rate changes of the various pacemaker models. The white shaded area is the SAN. SVC: superior rena cava, RAA: right atrium appendage, IVC: inferior vena cava, ISO: isoproterenol, RA: right atrium, Sup: superior, Sub: subsidiary pacemaker, inf: inferior, SAN: sinoatrial node.
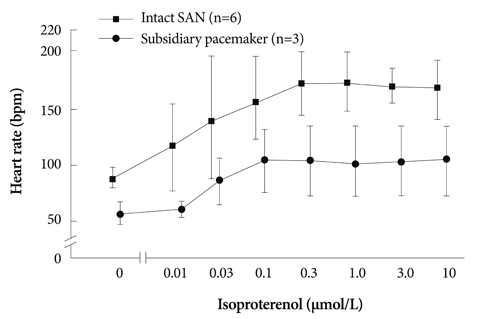
Fig. 3 Impaired isoproterenol-induced heart rate increase in the subsidiary pacemaker model. We tested the isoproterenol dose response curve in 6 RAs with an intact SAN and 3 subsidiary pacema-ker models. Compared to the RAs with an intact SAN (square), the subsidiary pacemaker model (circle) showed a significantly impaired heart rate increase during isoproterenol infusion. SAN: sinoatrial node, RA: right atrium.

Fig. 4 Isoproterenol response of the Langendorff-perfused RAs with an intact SAN. A: epicardial photographs of a perfused RA preparation with 3×3 cm optical fields of view. B: (a) baseline with a sinus rate of 94 bpm. (b) isoproterenol infusion of 1 µmol/L with a sinus rate of 160 bpm. Upper panels, RA Vm isochronal map. Lower panels, Cai and Vm tracings from the superior (S), mid (M) and inferior (I) SANs. Note the heart rate increase and shifting of the leading pacemaker site to the superior SAN with robust LDCAE (arrows). The earliest activation of the RA was considered as 0 ms. IVC: inferior vena cava, RAA: RA appendage, SVC: superior vena cava.

Fig. 5 Complete absence of LDCAE in the subsidiary PM model during isoproterenol infusion. A: epicardial photographs of a perfused right atrial preparation with 3×3 cm optical fields of view. B: the RA Vm isochronal map (upper panels) and the Cai and Vm tracings (lower panels) at baseline (a) and at the time of isoproterenol infusion (b). (a) Baseline with a heart rate of 60 bpm. (b) Isoproterenol infusion of 1 µmol/L with a sinus rate of 100 bpm. Cai and Vm tracings were recorded from the superior (S) and mid (M) SANs, and the earliest activation site of the subsidiary pacemaker (*). The stable subsidiary pacemaker was generated by ligation of the SAN artery. However, LDCAE was not observed at the earliest activation site of the subsidiary pacemaker. The earliest activation of RA was considered as 0 ms. IVC: inferior vena cava, RAA: RA appendage, SVC: superior vena cava, LDCAE: late diastolic Cai elevation, PM: paumaker, SAN: sinoatrial node.
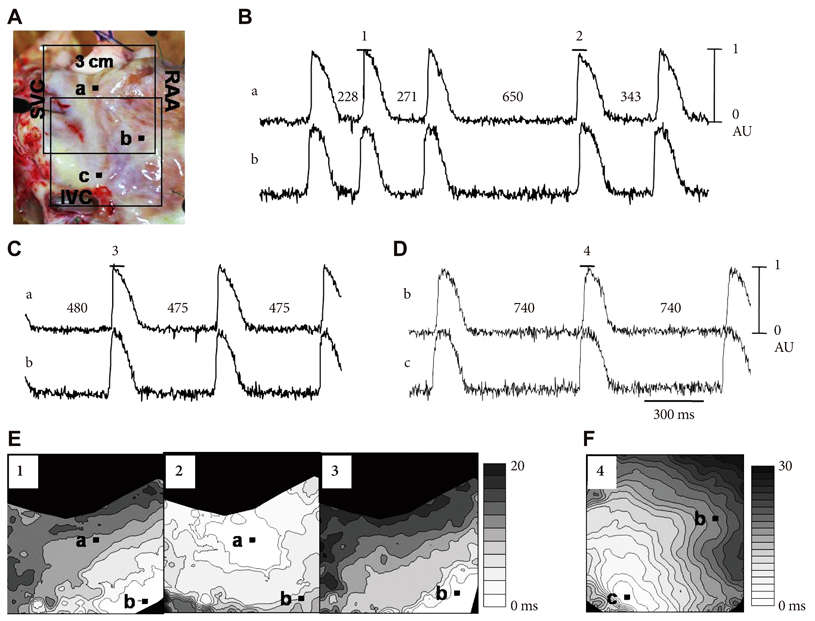
Fig. 6 Transient irregular rhythm after ligation of the superior part of the SAN artery. A: epicardial photographs of a perfused right atrial preparation with 3×3 cm optical fields of view. The upper and lower boxes present the optical fields of Fig. E and F, respectively. B and C, Vm tracings from the RA anterior (a) and superior CT (b) marked in Fig. E. B, Transient irregular rhythm immediately after SAN artery ligation. C: stable rhythm 10 minutes after SAN artery ligation. D: ryanodine infusion of 3 µmol/L. E: activation maps of the beats 1 and 2 (Fig. 6B) and 3 (Fig. 6C). F: shifting of the subsidiary pacemaker site to the inferior CT. The numbers on the Vm tracings of Fig. B to D present the beats from which the activation map was generated. IVC: inferior vena cava, RAA: RA appendage, SVC: superior vena cava.
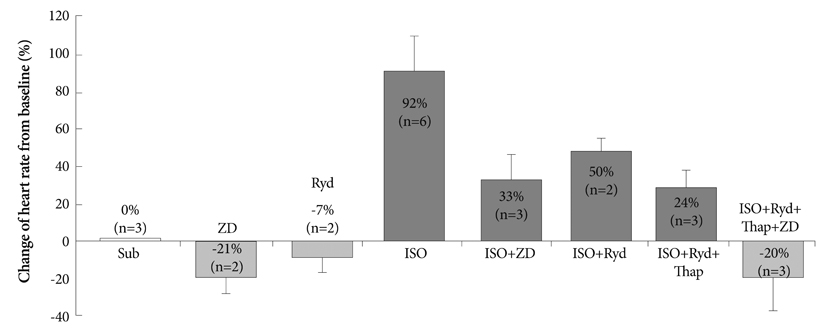
Fig. 7 Spontaneous heart rate of the subsidiary pacemaker depends upon both Ca2+-related mechanisms and the If current. The bars show a change in heart rate (% from baseline) induced by different pharmacological interventions. The black bars show the changes during 3 µmol/L ZD 7288, 3 µmol/L ryanodine, 10 µmol/L ryanodine plus 200 nmol/L thapsigargin infusion and 10 µmol/L ryanodine plus 200 nmol/L thapsigargin plus 3 µmol/L ZD 7288 infusion with 1 µmol/L ISO infusion. The grey bars show the changes during 3 µmol/L ZD 7288 and 3 µmol/L ryanodine without an ISO infusion. ISO: isoproterenol.
Reference
-
1. Adán V, Crown LA. Diagnosis and treatment of sick sinus syndrome. Am Fam Physician. 2003. 67:1725–1732.2. Randall WC, Talano J, Kaye MP, Euler D, Jones S, Brynjolfsson G. Cardiac pacemakers in absence of the SA node: responses to exercise and autonomic blockade. Am J Physiol. 1978. 234:H465–H470.3. Rozanski GJ, Lipsius SL, Randall WC. Functional characteristics of sinoatrial and subsidiary pacemaker activity in the canine right atrium. Circulation. 1983. 67:1378–1387.4. DiFrancesco D. Pacemaker mechanisms in cardiac tissue. Annu Rev Physiol. 1993. 55:455–472.5. DiFrancesco D. The pacemaker current (I(f)) plays an important role in regulating SA node pacemaker activity. Cardiovasc Res. 1995. 30:307–308.6. Hata T, Noda T, Nishimura M, Watanabe Y. The role of Ca2+ release from sarcoplasmic reticulum in the regulation of sinoatrial node automaticity. Heart Vessels. 1996. 11:234–241.7. Ju YK, Allen DG. Intracellular calcium and Na+-Ca2+ exchange current in isolated toad pacemaker cells. J Physiol. 1998. 508:153–166.8. Bogdanov KY, Vinogradova TM, Lakatta EG. Sinoatrial nodal cell ryanodine receptor and Na(+)-Ca(2+) exchanger: molecular partners in pacemaker regulation. Circ Res. 2001. 88:1254–1258.9. Vinogradova TM, Bogdanov KY, Lakatta EG. Beta-adrenergic stimulation modulates ryanodine receptor Ca(2+) release during diastolic depolarization to accelerate pacemaker activity in rabbit sinoatrial nodal cells. Circ Res. 2002. 90:73–79.10. Vinogradova TM, Zhou YY, Maltsev V, Lyashkov A, Stern M, Lakatta EG. Rhythmic ryanodine receptor Ca2+ releases during diastolic depolarization of sinoatrial pacemaker cells do not require membrane depolarization. Circ Res. 2004. 94:802–809.11. Vinogradova TM, Lyashkov AE, Zhu W, et al. High basal protein kinase A-dependent phosphorylation drives rhythmic internal Ca2+ store oscillations and spontaneous beating of cardiac pacemaker cells. Circ Res. 2006. 98:505–514.12. Joung B, Tang L, Maruyama M, et al. Intracellular calcium dynamics and acceleration of sinus rhythm by beta-adrenergic stimulation. Circulation. 2009. 119:788–796.13. Joung B, Ogawa M, Lin SF, Chen PS. The calcium and voltage clocks in sinoatrial node automaticity. Korean Circ J. 2009. 39:217–222.14. Joung B, Shinohara T, Zhang H, et al. Tachybradycardia in the isolated canine right atrium induced by chronic sympathetic stimulation and pacemaker current inhibition. Am J Physiol Heart Circ Physiol. 2010. 299:H634–H642.15. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias: the Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. N Engl J Med. 1997. 337:1576–1583.16. Joung BY, Koo BK, Xu ZZ, Kim IK, Lee MH, Kim US. The effects of obstacles on the dynamics of ventricular fibrillation. Korean Circ J. 2005. 35:183–191.17. Fedorov VV, Schuessler RB, Hemphill M, et al. Structural and functional evidence for discrete exit pathways that connect the canine sinoatrial node and atria. Circ Res. 2009. 104:915–923.18. Efimov IR, Fedorov VV, Joung B, Lin SF. Mapping cardiac pacemaker circuits: methodological puzzles of the sinoatrial node optical mapping. Circ Res. 2010. 106:255–271.19. Boineau JP, Schuessler RB, Mooney CR, et al. Multicentric origin of the atrial depolarization wave: the pacemaker complex: relation to dynamics of atrial conduction, P-wave changes and heart rate control. Circulation. 1978. 58:1036–1048.20. Boineau JP, Miller CB, Schuessler RB, et al. Activation sequence and potential distribution maps demonstrating multicentric atrial impulse origin in dogs. Circ Res. 1984. 54:332–347.21. Dobrzynski H, Boyett MR, Anderson RH. New insights into pacemaker activity: promoting understanding of sick sinus syndrome. Circulation. 2007. 115:1921–1932.22. Rubenstein DS, Lipsius SL. Mechanisms of automaticity in subsidiary pacemakers from cat right atrium. Circ Res. 1989. 64:648–657.23. Verheijck EE, vanKempen MJ, Veereschild M, Lurvink J, Jongsma HJ, Bouman LN. Electrophysiological features of the mouse sinoatrial node in relation to connexin distribution. Cardiovasc Res. 2001. 52:40–50.24. Lei M, Jones SA, Liu J, et al. Requirement of neuronal- and cardiac-type sodium channels for murine sinoatrial node pacemaking. J Physiol. 2004. 559:835–848.25. Lancaster MK, Jones SA, Harrison SM, Boyett MR. Intracellular Ca2+ and pacemaking within the rabbit sinoatrial node: heterogeneity of role and control. J Physiol. 2004. 556:481–494.26. Tellez JO, Dobrzynski H, Greener ID, et al. Differential expression of ion channel transcripts in atrial muscle and sinoatrial node in rabbit. Circ Res. 2006. 99:1384–1393.27. Efimov IR, Nikolski VP, Salama G. Optical imaging of the heart. Circ Res. 2004. 95:21–33.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Characteristics of Subsidiary Pacemaker in Complete Heartblock with Narrow QRS Complex
- Alterations of beta-Adrenergic Receptor Signaling in Cardiac Hypertrophy and Heart Failure: beta-Adrenergic Receptor Desensitization in Cardiac Disease
- The Effect of Beta-Adrenergic Receptor Blockade on the Atrial Refractory Period of Hyperthyroid Rabbits
- Function and Dysfunction of Human Sinoatrial Node
- A Case of Pacemaker Implantation in Premature Newborn with Congenital Complete Atrioventricular Block
