An Ileocutaneous Fistula That Developed 12 Years after Repair of an Abdominal Wall Defect Using Intraperitoneal Placement of High-density Polypropylene Mesh (Marlex(R))
- Affiliations
-
- 1Department of Urology, Chungju Hospital, Konkuk University College of Medicine, Cheongju, Korea.
- 2Department of Surgery, Chungju Hospital, Konkuk University College of Medicine, Cheongju, Korea. tulee@kku.ac.kr
- KMID: 2211271
- DOI: http://doi.org/10.4174/jkss.2009.76.2.119
Abstract
- Although prosthetic materials are commonly used to repair abdominal wall defects, they are also associated with postoperative complications. These complications could be prevented by the adoption of uniform guidelines on surgical methods and materials, but the best anatomical position for placement of prosthetic meshes is unclear. We report a case of an enterocutaneous fistula that developed after an abdominal wall defect was repaired by intraperitoneal application of a prosthetic mesh (Marlex(R)) to raise awareness of the consequences of improper use of prosthetic materials.
MeSH Terms
Figure
-
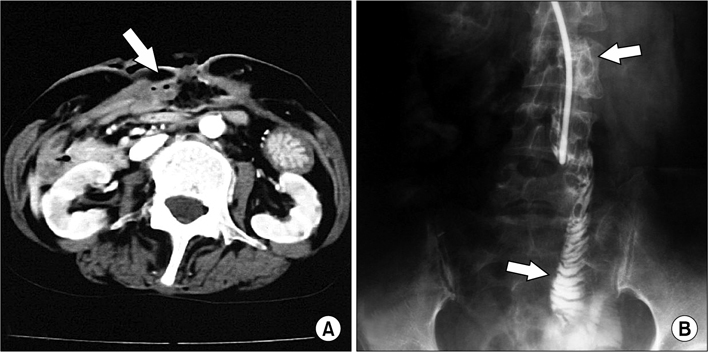
Fig. 1 (A) Abdominal spiral computed tomography (CT). This study revealed tubular structure, which was suspiciously thought to be part of the bowel, was protruded through the defect on the midline between rectus abdominis muscles. This suspicious bowel and adjacent parietal peritoneum showed diffused wall thickening and prominent enhancement. (B) Enterocutaneous fistulogram with Gastrografin for the confirmation of fistula between abdominal skin and ileum. Contrast material was identified at small bowel, but there was no extravasation or collection of contrast material through the fistula tract.
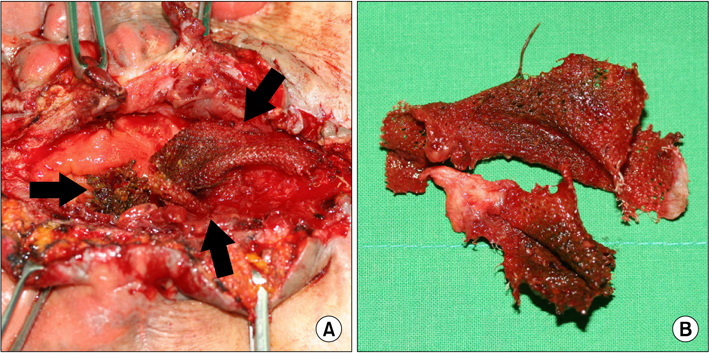
Fig. 2 (A) Intraoperative findings of laparotomy for previously indwelt intraperitoneal prosthetic mesh removal. (B) Removed polypropylene prosthetic meshes. These showed grayish, tan, and irregular soft tissue appearances. The larger removed mesh measures 7.8×4.5 cm and the others measure similarly.
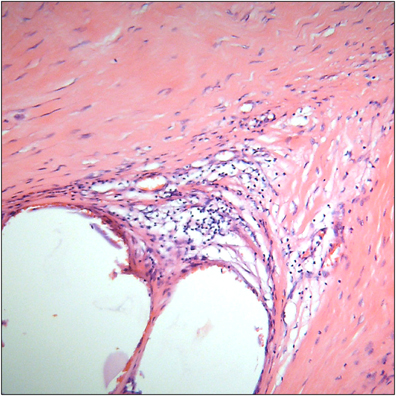
Fig. 3 Microscopic finding of the removed high-density polypropylene mesh. This is a plastic meshwork with foreign body reaction that contained inflamed granulation tissue and showed hemorrhagic and necrotizing inflammation (Hematoxylin-eosin stain, Magnification ×100).
Reference
-
1. Leber GE, Garb JL, Alexander AI, Reed WP. Long-term complications associated with prosthetic repair of incisional hernias. Arch Surg. 1998. 133:378–382.2. Halm JA, de Wall LL, Steyerberg EW, Jeekel J, Lange JF. Intraperitoneal polypropylene mesh hernia repair complicates subsequent abdominal surgery. World J Surg. 2007. 31:423–429.3. Losanoff JE, Richman BW, Jones JW. Entero-colocutaneous fistula: a late consequence of polypropylene mesh abdominal wall repair: case report and review of the literature. Hernia. 2002. 6:144–147.4. Engelsman AF, van der Mei HC, Ploeg RJ, Busscher HJ. The phenomenon of infection with abdominal wall reconstruction. Biomaterials. 2007. 28:2314–2327.5. Deysine M. Pathophysiology, prevention, and management of prosthetic infections in hernia surgery. Surg Clin North Am. 1998. 78:1105–1115.6. LeBlanc KA. Laparoscopic incisional and ventral hernia repair: complications-how to avoid and handle. Hernia. 2004. 8:323–331.7. Basoglu M, Yildirgan MI, Yilmaz I, Balik A, Celebi F, Atamanalp SS, et al. Late complications of incisional hernias following prosthetic mesh repair. Acta Chir Belg. 2004. 104:425–428.8. Vrijland WW, Jeekel J, Steyerberg EW, DenHoed PT, Bonjer HJ. Intraperitoneal polypropylene mesh repair of incisional hernia is not associated with enterocutaneous fistula. Br J Surg. 2000. 87:348–352.9. Bulic K, Dzepina I, Mijatovic D, Unusic J. Prosthetic mesh for infected abdominal wall defects? Report of a patient with a large full thickness abdominal wall defect and colostomy due to a gunshot wound. J Plast Reconstr Aesthet Surg. 2008. 61:455–458.10. Grevious MA, Cohen M, Shah SR, Rodriguez P. Structural and functional anatomy of the abdominal wall. Clin Plast Surg. 2006. 33:169–179.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transmural Mesh Migration From the Abdominal Wall to the Rectum After Hernia Repair Using a Prolene Mesh: A Case Report
- A Case of Traumatic Ventral Hernia Repair with a Porcine Dermal Collagen Graft (Permacol)
- A Comparison of Traditional Anterior Colporrhaphy and Cystocele Repair with Monofilament Polypropylene Mesh Repair (Gynemesh PSTM)
- Traumatic Abdominal Wall Hernia (TAWH): Repair by using a Prolen Mesh
- Comparison of Polypropylene Mesh and Expanded Polytetrafluoroethylene Patch for Repair of Abdominal Wall Defects in Rat
