J Korean Med Assoc.
2008 Dec;51(12):1087-1096. 10.5124/jkma.2008.51.12.1087.
Respiratory Diseases in Firefighters and Fire Exposers
- Affiliations
-
- 1Division of Respiratory Disease, Kyungpook National University College of Medicine, Korea. thjung@knu.ac.kr
- KMID: 2185968
- DOI: http://doi.org/10.5124/jkma.2008.51.12.1087
Abstract
- With the increasing use of synthetic chemical based products in building construction in recent decades, there has been growing concern over the health hazards to firefighters and fire exposers from the inhalation of the toxic components of smoke. Toxic combustion products can have profound effects on the respiratory system, causing symptoms, physiologic changes, and chronic diseases. Prompt evaluation is important and should include chest films, pulmonary function testing, arterial blood gas analysis, and bronchoscopy. Positive findings require aggressive management with adequate oxygenation, ventilation, pulmonary toilet, and fluid resuscitation. Clinicians caring for individuals who have sustained inhalation damage to their respiratory tract need to comprehensively understand the mechanisms, natural history, management, and prevention of acute inhalation injury, so that they can help individual patients recover without serious complications.
Keyword
MeSH Terms
Figure
-

Figure 1 Temporal evolution of smoke inhalation can be characterized by acute and chronic effects upon airways and lung parenchyma. Acute respiratory injuries may resolve completely or, less often, lead to permanent dysfunction (4).
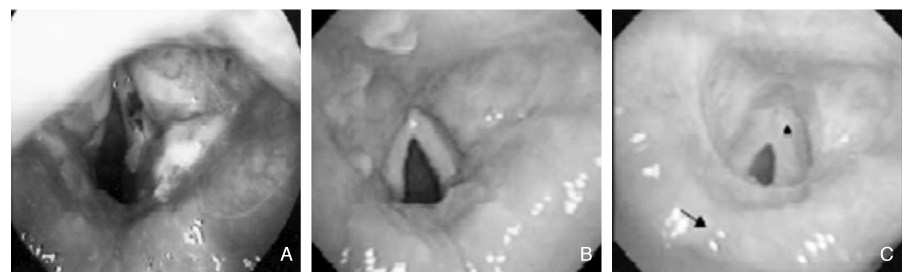
Figure 2 Laryngoscopic findings 3 (A); 16 (B); and 78 (C) days after extubation, showing posterior commissure stenosis (arrow) of the vocal cords, with anterior adhesion (arrowhead) (3).
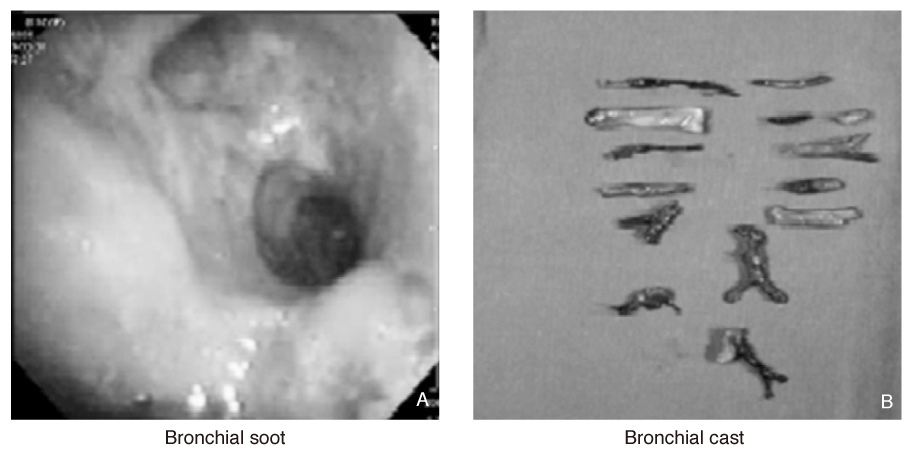
Figure 3 Bronchial soot (A) on bronchoscopy and bronchial casts (B) removed from one fire victim (3).
Reference
-
1. Rabinowitz PM, Siegel MD. Acute inhalation injury. Clin Chest Med. 2002. 23:707–715.
Article2. Saffle JR. The 1942 fire at Boston's Cocoanut Grove nightclub. Am J Surg. 1993. 166:581–591.
Article3. Cha SI, Kim CH, Lee JH, Park JY, Jung TH, Choi WI, Choi WI, Han SB, Jeon YJ, Shin KC, Chung JH, Lee KH, Kim YJ, Lee BK. Isolated smoke inhalation injuries: acute respiratory dysfunction, clinical outcomes, and short-term evolution of pulmonary functions with the effects of steroids. Burns. 2007. 33:200–208.
Article4. Haponik EF. Clinical smoke inhalation injury: pulmonary effects. Occup Med. 1993. 8:430–468.5. Young CJ, Moss J. Smoke inhalation: diagnosis and treatment. J Clin Anesth. 1989. 1:377–386.
Article6. Trunkey DD. Inhalation injury. Surg Clin North Am. 1978. 58:1133–1140.
Article7. Summer W, Haponik E. Inhalation of irritant gases. Clin Chest Med. 1981. 2:273–287.
Article8. Alarie Y. Toxicity of fire smoke. Crit Rev Toxicol. 2002. 32:259–289.
Article9. Clark WR. Smoke inhalation:diagnosis and treatment. World J Surg. 1992. 16:24–29.10. Heimbach DM, Waeckerle JF. Inhalation injury. Ann Int Med. 1988. 17:1316–1320.11. Lee-Chiong TL Jr. Smoke inhalation injury, when to suspect and how to treat. Postgrad Med. 1999. 105:55–62.12. Clark CJ, Pollock AJ, Reid WH, Campbell D, Gemmell C. Role of pulmonary alveolar macrophage activation in acute lung injury after burns and smoke inhalation. Lancet. 1988. 2:872–874.
Article13. Lykens MG, Haponik EF, Meredith SH, Bass DA. Survival after acute thermal inhalation injury: Clinical and BAL predictors. Am Rev Respir Dis. 1992. 145:417.14. Bullard JE, Koepsell TD, Rivara F. Association of smoking and alcohol drinking with residential fire injuries. Am J Epidemiol. 1992. 135:26–34.
Article15. Choe JY, Cho YG, Kweon S, Lee WS, Jung TH. Arterial blood gas analyses in patients with acute carbon monoxide poisoning. Korean J Med. 1989. 36:247–253.16. Fogarty PW, George PJ, Solomon M, Spiro SG, Armstrong RF. Long term effects of smoke inhalation in survivors of the King's Cross underground station fire. Thorax. 1991. 46:914–918.
Article17. Lund T, Goodwin CW, McManus WF, Shirani KZ, Stallings RJ, Mason AD Jr, Pruitt BA Jr. Upper airway sequelae in burn patients requiring endotracheal intubation or tracheostomy. Ann Surg. 1985. 201:374–382.
Article18. Park GY, Park JW, Jeong DH, Jeong SH. Prolonged airway and systemic inflammatory reactions after smoke inhalation. Chest. 2003. 123:475–480.
Article19. Tasaka S, Kanazawa M, Mori M, Fujishima S, Ishizaka A, Yamasawa F, Kawashiro T. Long-term course of bronchiectasis and bronchiolitis obliterans as late complication of smoke inhalation. Respiration. 1995. 62:40–42.
Article20. Wright JL. Inhalational lung injury causing bronchiolitis. Clin Chest Med. 1993. 14:635–644.
Article21. Boulet LP. Increases in airway responsiveness following acute exposure to respiratory irritants. Reactive airway dysfunction syndrome or occupational asthma. Chest. 1988. 94:476–481.
Article22. Liu D, Tager IB, Balmes JR, Harrison RJ. The effect of smoke inhalation on lung function and airway responsiveness in wildland fire fighters. Am Rev Respir Dis. 1992. 146:1469–1473.
Article23. Banauch GI, Alleyne D, Sanchez R, Olender K, Cohen HW, Weiden M, Kelly KJ, Prezant DJ. Persistent hyperreactivity and reactive airway dysfunction in firefighters at the World Trade Center. Am J Respir Crit Care Med. 2003. 168:54–62.
Article24. Baud FJ, Barriot P, Toffis V, Riou B, Vicaut E, Lecarpentier Y, Bourdon R, Astier A, Bismuth C. Elevated blood cyanide concentrations in victims of smoke inhalation. N Engl J Med. 1991. 325:1761–1766.
Article25. Clark CJ, Campbell D, Reid WH. Blood carboxyhaemoglobin and cyanide levels in fire survivors. Lancet. 1981. 1:1332–1335.
Article26. Barie PS, Wu W, Hariri RJ, Halebian PH, Shires GT. Alterations of pulmonary gas exchange after superimposed carbon monoxide poisoning in acute lung injury. Surgery. 1994. 115:678–686.27. Texidor HS, Rubin E, Novick GS, Alonso DR. Smoke inhalation: radiologic manifestation. Radiology. 1983. 149:383–387.28. Freitag L, Firusian N, Stamatis G, Greschuchna D. The role of bronchoscopy in pulmonary complication due to mustard gas inhalation. Chest. 1991. 100:1436–1441.
Article29. Jung TH. Practical bronchoscopy. Korean J Med. 1998. 55:738–751.30. Whitener DR, Whitener LM, Robertson KJ, Baxter CR, Pierce AK. Pulmonary function measurements in patients with thermal injury and smoke inhalation. Am Rev Respir Dis. 1980. 122:731–739.
Article31. Jung TH. Interpretation of spirometry and flow-volume curve. Tuberc Respir Dis. 1991. 38:413–430. (Korean).32. Rogers SN, Benumof JL. New and easy techniques for fiberoptic endoscopy-aided tracheal intubation. Anesthesiology. 1983. 59:569–572.
Article33. Navar PD, Saffle JR, Warden GD. Effect of inhalation injury on fluid resuscitation requirements after thermal injury. Am J Surg. 1985. 150:716–720.
Article34. Davies LK, Poulton TJ, Modell JH. Continuous positive airway pressure is beneficial in treatment of smoke inhalation. Crit Care Med. 1983. 11:726–729.
Article35. Venus B, Matsuda T, Copiozo JB, Mathru M. Prophylactic intubation and continuous positive airway pressure in the management of inhalation injury in burn victims. Crit Care Med. 1981. 9:519–523.
Article36. Robinson NB, Hudson LD, Riem M, Miller E, Willoughby J, Ravenholt O, Carrico CJ, Heimbach DM. Steroid therapy following isolated smoke inhalation injury. J Trauma. 1982. 22:876–879.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Function and Respiratory Symptoms of Municipal Fire Officers in Busan.
- Cancer Perceptions Among Smokeless Tobacco Users: A Qualitative Study of US Firefighters
- Hospital admissions due to endocrine diseases in Korean male firefighters
- The “Warm Zone†Cases: Environmental Monitoring Immediately Outside the Fire Incident Response Arena by Firefighters
- Cardiovascular Disease, Cancer and Reproductive Hazards in Firefighters
