Insulin Secretion and Insulin Resistance in Newly Diagnosed, Drug Naive Prediabetes and Type 2 Diabetes Patients With/Without Metabolic Syndrome
- Affiliations
-
- 1Department of Endocrinology and Metabolism, School of Medicine, Kyung Hee University, Korea.
- 2Research Institute of Endocrinology, School of Medicine, Kyung Hee University, Korea.
- KMID: 2177614
- DOI: http://doi.org/10.4093/jkda.2006.30.3.198
Abstract
-
BACKGROUND: To evaluate the relationships between deterioration in insulin secretion and aggravated insulin resistance in patients with newly diagnosed prediabetes (preDM) and type 2 diabetes mellitus (T2DM) according to the presence of metabolic syndrome (MS).
METHODS
We performed oral glucose tolerance test (OGTT) on 322 drug naive subjects with a history of hyperglycemia of < or = 3 months, and divided these patients into 3 groups, normal glucose tolerance (NGT), preDM (IFG and/or IGT) and T2DM. We also diagnosed these subjects with respect to MS according to ATP III criteria modified by Asia-Pacific guidelines and compared IGI and HOMA-IR in the 3 groups.
RESULTS
According to OGTT, 63 subjects were diagnosed with NGT, 81 with preDM, and 178 with T2DM. Using modified ATP III criteria, 218 (67.7%) subjects were diagnosed as MS. When compare groups stratified by the presence of MS, preDM and T2DM groups with MS showed significantly higher mean HOMA-IR and IGI than those without MS. When compare groups with respect to glucose tolerance, NGT, preDM, and T2DM subgroups in MS group showed significant higher HOMA-IR and lower IGI according to glucose tolerance. However, NGT, preDM, and T2DM subgroups in non-MS group showed a significant decrease in IGI but no significant difference in HOMA-IR as glucose tolerance worsened.
CONCLUSION
Deterioration in IGI and aggravation of HOMA-IR are both important in the primary pathogenesis of diabetes in those with MS. However, IGI deterioration may be the only important factor in the primary pathogenesis of T2DM in the absence of MS.
MeSH Terms
Figure
-
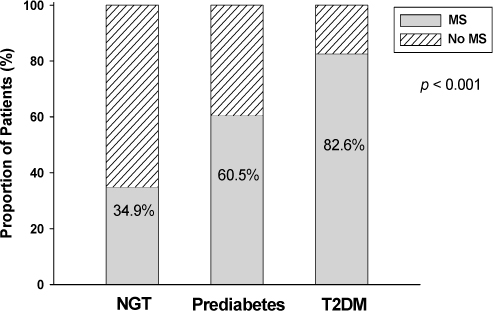
Fig. 1 Prevalence of Metabolic syndrome among study subjects.
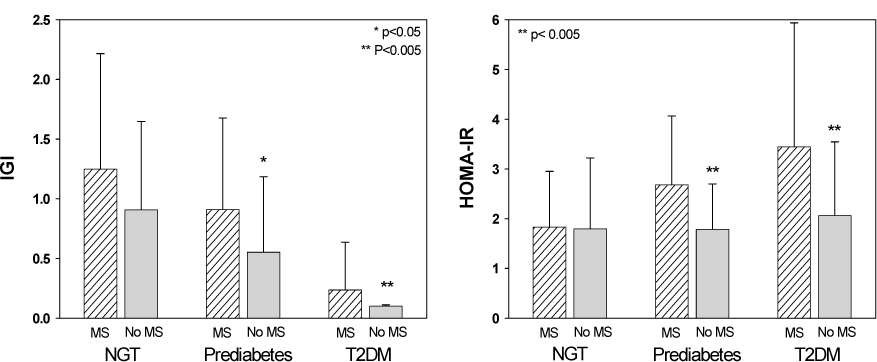
Fig. 2 IGI and HOMA-IR differences according to the presence of MS in the three glucose tolerance subgroups. Both IGI and HOMA-IR were significantly elevated in MS subgroups.
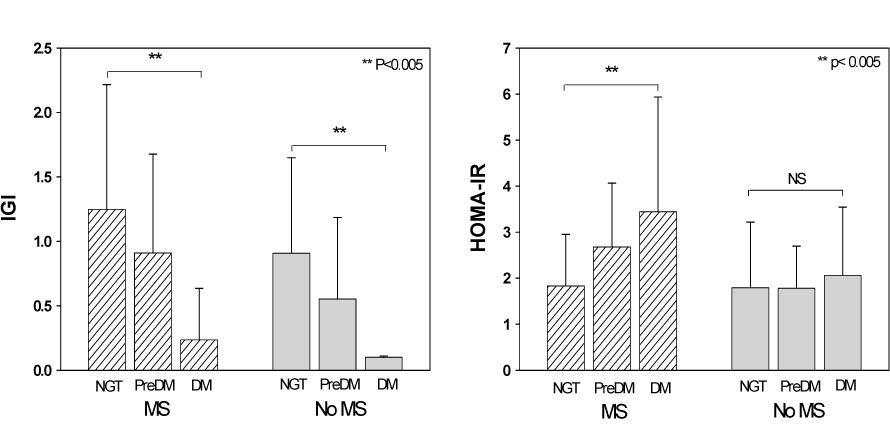
Fig. 3 Differences in IGI and HOMA-IR according to glucose tolerance in patients with/without MS. In MS patients, IGI values progressively decreased and HOMA-IR values progressively increased with increased glucose tolerance aggravation. However, though IGI values progressively decreased in patients without MS with increasing glucose tolerance aggravation, HOMA-IR values were unaffected.

Fig. 4 Hypothesis concerning primary metabolic changes during the development of type 2 DM. In patients with MS, IGI (compensatory insulin secretion) deterioration and HOMA-IR (insulin resistance) aggravation are both important in the primary pathogenesis of diabetes. However, HOMA-IR aggravation may not be an important factor in the pathogenesis of diabetes in those without MS.
Reference
-
1. DeFronzo RA. Pathogenesis of type 2 diabetes mellitus. Med Clin North Am. 2004. 88:787–835. IX2. Kahn SE. Clinical review 135: The importance of beta-cell failure in the development and progression of type 2 diabetes. J Clin Endocrinol Metab. 2001. 86:4047–4058.3. Leahy JL. Natural history of beta-cell dysfunction in NIDDM. Diabetes Care. 1990. 13:992–1010.4. Weyer C, Bogardus C, Mott DM, Pratley RE. The natural history of insulin secretory dysfunction and insulin resistance in the pathogenesis of type 2 diabetes mellitus. J Clin Invest. 1999. 104:787–794.5. Hawkins M, Rossetti L. Insulin Resistance and Its Role in the Pathogenesis of Type 2 Diabetes. 2005. Lippincott Willians & Wilkins.6. Folsom AR, Kushi LH, Anderson KE, Mink PJ, Olson JE, Hong CP, Sellers TA, Lazovich D, Prineas RJ. Associations of general and abdominal obesity with multiple health outcomes in older women: the Iowa Women's Health Study. Arch Intern Med. 2000. 160:2117–2128.7. Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW Jr. Body-mass index and mortality in a prospective cohort of U.S. adults. N Engl J Med. 1999. 341:1097–1105.8. Lillioja S, Mott DM, Spraul M, Ferraro R, Foley JE, Ravussin E, Knowler WC, Bennett PH, Bogardus C. Insulin resistance and insulin secretory dysfunction as precursors of non-insulin-dependent diabetes mellitus. Prospective studies of Pima Indians. N Engl J Med. 1993. 329:1988–1992.9. Martin BC, Warram JH, Krolewski AS, Bergman RN, Soeldner JS, Kahn CR. Role of glucose and insulin resistance in development of type 2 diabetes mellitus: results of a 25-year follow-up study. Lancet. 1992. 340:925–929.10. Meigs JB. Invited commentary: insulin resistance syndrome? Syndrome X? Multiple metabolic syndrome? A syndrome at all? Factor analysis reveals patterns in the fabric of correlated metabolic risk factors. Am J Epidemiol. 2000. 152:908–911. discussion 912.11. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001. 285:2486–2497.12. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA. 2002. 287:356–359.13. Tripathy D, Carlsson M, Almgren P, Isomaa B, Taskinen MR, Tuomi T, Groop LC. Insulin secretion and insulin sensitivity in relation to glucose tolerance: lessons from the Botnia Study. Diabetes. 2000. 49:975–980.14. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2004. 27:Suppl 1. S5–S10.15. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985. 28:412–419.16. The IDF consensus worldwide definition of the metabolic syndrome [article online]. 2005. Available from http://www.idf.org/webdata/docs/IDF_Metasyndrome_definition.pdfhttp://www.idf.org/webdata/docs/IDF_Metasyndrome_definition.pdf.17. Lee WY, Park JS, Noh SY, Rhee EJ, Kim SW, Zimmet PZ. Prevalence of the metabolic syndrome among 40,698 Korean metropolitan subjects. Diabetes Res Clin Pract. 2004. 65:143–149.18. Yeckel CW, Taksali SE, Dziura J, Weiss R, Burgert TS, Sherwin RS, Tamborlane WV, Caprio S. The normal glucose tolerance continuum in obese youth: evidence for impairment in beta-cell function independent of insulin resistance. J Clin Endocrinol Metab. 2005. 90:747–754.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Retraction: Insulin Secretion and Insulin Resistance in Newly Diagnosed, Drug Naive Prediabetes and Type 2 Diabetes Patients With/Without Metabolic Syndrome
- Insulin Resistance Changes after Metabolic/Bariatric Surgery
- The Changes in Early Phase Insulin Secretion in Newly Diagnosed, Drug Naive Korean Prediabetes Subjects
- Insulin Resistance in Polycystic Ovary Syndrome
- Changing Clinical Characteristics according to Insulin Resistance and Insulin Secretion in Newly Diagnosed Type 2 Diabetic Patients in Korea
