Investig Magn Reson Imaging.
2015 Mar;19(1):31-36. 10.13104/imri.2015.19.1.31.
Contrast-enhanced Magnetic Resonance Imaging of Brain Metastases at 7.0T versus 1.5T: A Preliminary Result
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Hospital, Cancer Research Institute, Ischemic/Hypoxic Disease Institute, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Radiology, Seoul National University College of Medicine, Seoul, Korea. neurorad63@gmail.com
- 3Neuroscience Research Institute, Gachon University of Medicine and Science, Incheon, Korea.
- KMID: 2175574
- DOI: http://doi.org/10.13104/imri.2015.19.1.31
Abstract
- PURPOSE
To compare the depiction of brain metastases on contrast-enhanced images with 7.0 tesla (T) and at 1.5T MRI.
MATERIALS AND METHODS
Four consecutive patients with brain metastases were scanned on 7.0T whole-body scanner and 1.5T MRI. A 3D T1-weighted gradient echo sequence (3D T1-GRE) at 1.5T (voxel size = 0.9 x 0.9 x 1.5 mm3 after double-dose, gadoterate meglumine, Gd-DOTA) was compared to a 7.0T 3D T1-GRE sequence (voxel size = 0.4 x 0.4 x 0.8 mm3, single-dose Gd-DOTA) in four patients after a 5 minute delay. The number of contrast-enhancing metastases in MPRAGE images was compared in each patient by two radiologists in consensus. We measured contrast ratio of enhancing brain metastases and white matter in 1.5T and 7.0T.
RESULTS
In all four patients 7.0T 3D T1-GRE images after single-dose Gd-DOTA and 1.5T after double-dose Gd-DOTA depicted 11 brain metastases equally. In the quantitative analysis of contrast ratios of enhancing brain metastases and white matter, the 1.5T 3D T1-GRE after double-dose showed an increased contrast ratio compared to 7.0T 3D T1-GRE after single-dose (0.961 +/- 0.571 versus 0.885 +/- 0.494; n = 11 metastases). But this difference was not statistically significant (P = 0.711).
CONCLUSION
Our preliminary results indicate that 7.0T single-dose Gd-enhanced images were not different to 1.5T double-dose Gd-enhanced images for the detection of brain metastases.
Keyword
Figure
-

Fig. 1 63-years-old woman with single brain metastasis from lung adenocarcinoma. Double-dose Gd-enhanced axial 3D T1-GRE image shows a ring like enhancing lesion at the right precentral gyrus at 1.5T (a), and single-dose Gd-enhanced 3D T1-GRE image clearly demonstrates the peripheral enhancing rim portion of the metastasis at 7.0T (b).
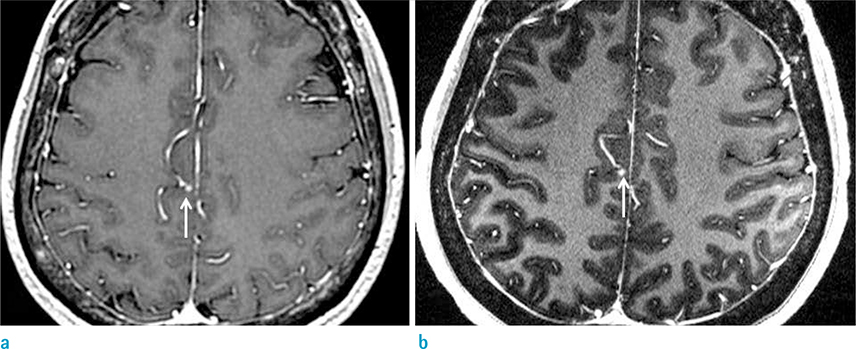
Fig. 2 56-years-old woman with five brain metastases from lung adenocarcinoma. A right paracentral lobule metastasis (white arrow) has similar signal intensity at 1.5T double-dose (a) and 7.0T single-dose (b) Gd-based axial T1-GRE images (mean tumor-brain contrast ratio 0.604/0.611 = 1.5T/7.0T).
Reference
-
1. Klos KJ, O'Neill BP. Brain metastases. Neurologist. 2004; 10:31–46.2. Arnold SM, Patchell RA. Diagnosis and management of brain metastases. Hematol Oncol Clin North Am. 2001; 15:1085–1107. vii.3. Sanchez de Cos J, Sojo Gonzalez MA, Montero MV, Perez Calvo MC, Vicente MJ, Valle MH. Non-small cell lung cancer and silent brain metastasis. Survival and prognostic factors. Lung Cancer. 2009; 63:140–145.4. Smalley SR, Schray MF, Laws ER Jr, O'Fallon JR. Adjuvant radiation therapy after surgical resection of solitary brain metastasis: association with pattern of failure and survival. Int J Radiat Oncol Biol Phys. 1987; 13:1611–1616.5. Davis PC, Hudgins PA, Peterman SB, Hoffman JC Jr. Diagnosis of cerebral metastases: double-dose delayed CT vs contrast-enhanced MR imaging. AJNR Am J Neuroradiol. 1991; 12:293–300.6. Engh JA, Flickinger JC, Niranjan A, Amin DV, Kondziolka DS, Lunsford LD. Optimizing intracranial metastasis detection for stereotactic radiosurgery. Stereotact Funct Neurosurg. 2007; 85:162–168.7. Jena A, Taneja S, Talwar V, Sharma JB. Magnetic resonance (MR) patterns of brain metastasis in lung cancer patients: correlation of imaging findings with symptom. J Thorac Oncol. 2008; 3:140–144.8. Runge VM, Kirsch JE, Burke VJ, et al. High-dose gadoteridol in MR imaging of intracranial neoplasms. J Magn Reson Imaging. 1992; 2:9–18.9. Sze G, Johnson C, Kawamura Y, et al. Comparison of single- and triple-dose contrast material in the MR screening of brain metastases. AJNR Am J Neuroradiol. 1998; 19:821–828.10. Hawighorst H, Debus J, Schreiber W, et al. Contrast-enhanced magnetization transfer imaging: improvement of brain tumor conspicuity and delineation for radiosurgical target volume definition. Radiother Oncol. 1997; 43:261–267.11. Komada T, Naganawa S, Ogawa H, et al. Contrast-enhanced MR imaging of metastatic brain tumor at 3 tesla: utility of T(1)-weighted SPACE compared with 2D spin echo and 3D gradient echo sequence. Magn Reson Med Sci. 2008; 7:13–21.12. Trattnig S, Pinker K, Ba-Ssalamah A, Nobauer-Huhmann IM. The optimal use of contrast agents at high field MRI. Eur Radiol. 2006; 16:1280–1287.13. Paek SH, Son YD, Chung HT, Kim DG, Cho ZH. Clinical application of 7.0 T magnetic resonance images in Gamma Knife radiosurgery for a patient with brain metastases. J Korean Med Sci. 2011; 26:839–843.14. Yuh WT, Christoforidis GA, Koch RM, et al. Clinical magnetic resonance imaging of brain tumors at ultrahigh field: a state-of-the-art review. Top Magn Reson Imaging. 2006; 17:53–61.15. Nobauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. Magnetic resonance imaging contrast enhancement of brain tumors at 3 tesla versus 1.5 tesla. Invest Radiol. 2002; 37:114–119.16. Schwindt W, Kugel H, Bachmann R, et al. Magnetic resonance imaging protocols for examination of the neurocranium at 3 T. Eur Radiol. 2003; 13:2170–2179.17. Krautmacher C, Willinek WA, Tschampa HJ, et al. Brain tumors: full- and half-dose contrast-enhanced MR imaging at 3.0 T compared with 1.5 T--Initial Experience. Radiology. 2005; 237:1014–1019.18. Pfeuffer J, van de Moortele PF, Yacoub E, et al. Zoomed functional imaging in the human brain at 7 Tesla with simultaneous high spatial and high temporal resolution. Neuroimage. 2002; 17:272–286.19. Vaughan JT, Garwood M, Collins CM, et al. 7T vs. 4T: RF power, homogeneity, and signal-to-noise comparison in head images. Magn Reson Med. 2001; 46:24–30.20. Ugurbil K, Adriany G, Andersen P, et al. Ultrahigh field magnetic resonance imaging and spectroscopy. Magn Reson Imaging. 2003; 21:1263–1281.21. Gizewski ER, de Greiff A, Maderwald S, Timmann D, Forsting M, Ladd ME. fMRI at 7 T: whole-brain coverage and signal advantages even infratentorially? Neuroimage. 2007; 37:761–768.22. Biswas J, Nelson CB, Runge VM, et al. Brain tumor enhancement in magnetic resonance imaging: comparison of signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) at 1.5 versus 3 tesla. Invest Radiol. 2005; 40:792–797.23. Lupo JM, Banerjee S, Hammond KE, et al. GRAPPA-based susceptibility-weighted imaging of normal volunteers and patients with brain tumor at 7 T. Magn Reson Imaging. 2009; 27:480–488.24. Monninghoff C, Maderwald S, Theysohn JM, et al. Imaging of brain metastases of bronchial carcinomas with 7 T MRI - initial results. Rofo. 2010; 182:764–772.25. Yuh WT, Tali ET, Nguyen HD, Simonson TM, Mayr NA, Fisher DJ. The effect of contrast dose, imaging time, and lesion size in the MR detection of intracerebral metastasis. AJNR Am J Neuroradiol. 1995; 16:373–380.26. Akeson P, Larsson EM, Kristoffersen DT, Jonsson E, Holtas S. Brain metastases--comparison of gadodiamide injection-enhanced MR imaging at standard and high dose, contrast-enhanced CT and non-contrast-enhanced MR imaging. Acta Radiol. 1995; 36:300–306.27. Broome DR, Girguis MS, Baron PW, Cottrell AC, Kjellin I, Kirk GA. Gadodiamide-associated nephrogenic systemic fibrosis: why radiologists should be concerned. AJR Am J Roentgenol. 2007; 188:586–592.28. Sadowski EA, Bennett LK, Chan MR, et al. Nephrogenic systemic fibrosis: risk factors and incidence estimation. Radiology. 2007; 243:148–157.29. Thomsen HS. Nephrogenic systemic fibrosis: A serious late adverse reaction to gadodiamide. Eur Radiol. 2006; 16:2619–2621.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- T2 Relaxation Times of the Cingulate Cortex, Amygdaloid Body, Hippocampal Body, and Insular Cortex: Comparison of 1.5 T and 3.0 T
- MR imaging of intracerebral hemorrhagic lesions: comparison of 2.0 T and 0.5 T images
- A Case Report of Preoperative and Postoperative 7.0T Brain MRI in a Patient with a Small Cell Glioblastoma
- Contrast-enhanced Fast Fluid-attenuated Inversion Recovery MR Imaging in Patients with Brain Tumors
- Does Multiphasic Contrast Enhanced Fluid Attenuated Inversion Recovery Magnetic Resonance Imaging Enhance the Detectability of Small Intracerebral Metastases?
