Coexistence of Solitary Rectal Ulcer Syndrome and Ulcerative Colitis: A Case Report and Literature Review
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. yejoo@chonnam.ac.kr
- KMID: 2174341
- DOI: http://doi.org/10.5217/ir.2014.12.1.70
Abstract
- Solitary rectal ulcer syndrome (SRUS) is an uncommon benign disease that is misdiagnosed as malignancy or inflammatory bowel disease because of similarities in clinical and endoscopic manifestations. Furthermore, SRUS with ulcerative colitis (UC) is extremely rare. To date, two cases have been reported in the medical literature. We report an additional case of SRUS with UC that was misdiagnosed as rectal cancer. A 61-year-old man was admitted to our hospital with rectal bleeding. Colonoscopy showed a well-demarcated, shallow, ulcerative lesion with polypoidal growth involving the entire circumference of the rectal lumen. Findings from imaging studies, including abdominal computed tomography (CT) and positron emission tomography (PET)/CT resembled those of rectal cancer. Surgical resection was performed because clinical symptoms persisted despite medical treatment and because occult rectal cancer could not be ruled out. Histopathological examination of the resected specimen revealed fibromuscular obliteration of the lamina propria and crypt abscesses, characteristics compatible with SRUS and UC.
MeSH Terms
Figure
-
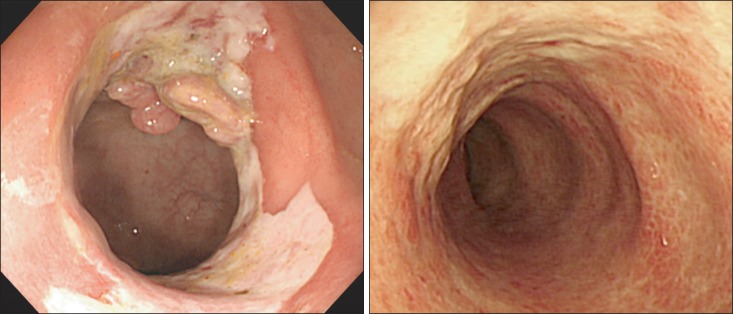
Fig. 1 Colonoscopic findings. Colonoscopy shows a well-demarcated, shallow ulcerative lesion with polypoid growth involving the entire circumference of the rectal lumen (A). In addition, loss of vascular pattern and the presence of mucopus coating and edema were noted (B).
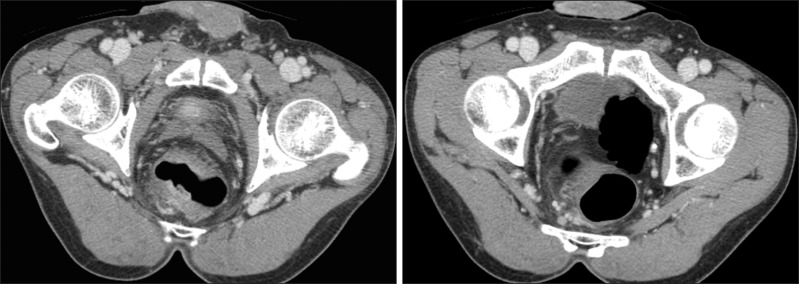
Fig. 2 Abdominal CT findings. CT reveals concentric wall thickening with enhancement in the rectum (A) and enlargement of the regional lymph nodes (B).
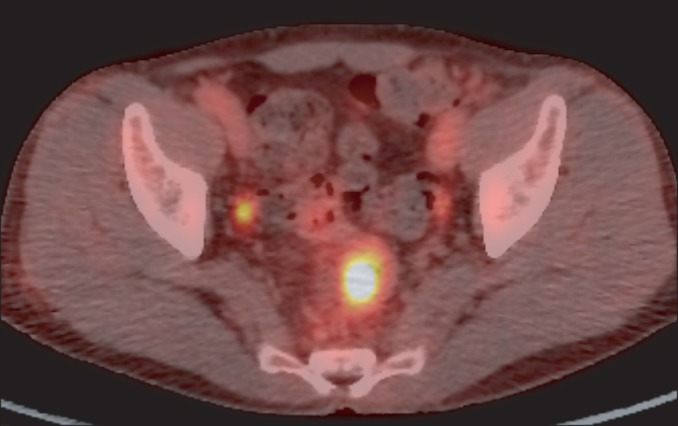
Fig. 3 Fluorine-18-fluorodeoxyglucose (FDG)-positron emission tomography/CT findings. PET/CT reveals increased FDG uptake in the rectum and regional lymph nodes.

Fig. 4 Histopathological findings of the rectum. Histopathological examination of the resected specimen reveals thickening of the muscularis mucosa and fibromuscular obliteration of the lamina propria (A). Crypt abscesses, focal gland destruction, and increased inflammatory cells in the lamina propria are also seen (B) (H&E stain, ×100).
Reference
-
1. Tjandra JJ, Fazio VW, Church JM, Lavery IC, Oakley JR, Milsom JW. Clinical conundrum of solitary rectal ulcer. Dis Colon Rectum. 1992; 35:227–234. PMID: 1740066.
Article2. Ho YH, Ho JM, Parry BR, Goh HS. Solitary rectal ulcer syndrome: the clinical entity and anorectal physiological findings in Singapore. Aust N Z J Surg. 1995; 65:93–97. PMID: 7857237.
Article3. Beck DE. Surgical therapy for colitis cystica profunda and solitary rectal ulcer syndrome. Curr Treat Options Gastroenterol. 2002; 5:231–237. PMID: 12003718.
Article4. Li SC, Hamilton SR. Malignant tumors in the rectum simulating solitary rectal ulcer syndrome in endoscopic biopsy specimens. Am J Surg Pathol. 1998; 22:106–112. PMID: 9422323.
Article5. Sharara AI, Azar C, Amr SS, Haddad M, Eloubeidi MA. Solitary rectal ulcer syndrome: endoscopic spectrum and review of the literature. Gastrointest Endosc. 2005; 62:755–762. PMID: 16246692.6. Chong VH, Jalihal A. Solitary rectal ulcer syndrome: characteristics, outcomes and predictive profiles for persistent bleeding per rectum. Singapore Med J. 2006; 47:1063–1068. PMID: 17139403.7. Tjandra JJ, Fazio VW, Petras RE, et al. Clinical and pathologic factors associated with delayed diagnosis in solitary rectal ulcer syndrome. Dis Colon Rectum. 1993; 36:146–153. PMID: 8425418.
Article8. Madigan MR, Morson BC. Solitary ulcer of the rectum. Gut. 1969; 10:871–881. PMID: 5358578.
Article9. Niv Y, Bat L. Solitary rectal ulcer syndrome-clinical, endoscopic, and histological spectrum. Am J Gastroenterol. 1986; 81:486–491. PMID: 3706271.10. Chiang JM, Changchien CR, Chen JR. Solitary rectal ulcer syndrome: an endoscopic and histological presentation and literature review. Int J Colorectal Dis. 2006; 21:348–356. PMID: 16133006.11. Saul SH, Sollenberger LC. Solitary rectal ulcer syndrome. Its clinical and pathological underdiagnosis. Am J Surg Pathol. 1985; 9:411–421. PMID: 4091179.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Solitary Rectal Ulcer Syndrome with Lesion of Polypoid Growth
- A Case of Solitary Rectal Ulcer Syndrome
- Two Cases of Atypical Ulcerative Colitis - Rectal Sparing Ulcerative Colitis Associated with Primary Sclerosing Cholangitis -
- Malignant change of chronic ulcerative colitis : report of a case
- A Case of Cytomegalvirus Colitis Developed during the Treatment of Ulcerative Colitis
