Cancer Res Treat.
2016 Jan;48(1):259-265. 10.4143/crt.2014.370.
An Alternative Triage Strategy Based on Preoperative MRI for Avoiding Trimodality Therapy in Stage IB Cervical Cancer
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Institute of Women's Life Medical Science, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Obstetrics and Gynecology, Seoul National University College of Medicine, Seoul, Korea. kjwksh@snu.ac.kr
- 3Department of Obstetrics and Gynecology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 4Department of Radiation Oncology, Seoul National University College of Medicine, Seoul, Korea.
- 5Department of Radiology, Seoul National University College of Medicine, Seoul, Korea.
- 6Department of Pathology, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2152283
- DOI: http://doi.org/10.4143/crt.2014.370
Abstract
- PURPOSE
Adjuvant chemoradiation following primary surgery is frequently indicated in patients with stage IB cervical cancer. The aim of this study is to evaluate the role of a magnetic resonance imaging (MRI)-based strategy in avoiding trimodality therapy.
MATERIALS AND METHODS
We retrospectively reviewed all patients with stage IB cervical cancer treated initially with primary surgery at Seoul National University Hospital. We suggest an alternative triage strategy in which the primary treatment modality is determined based on preoperative MRI findings. Using this strategy, primary surgery is only indicated when there is no evidence of parametrial involvement (PMI) and lymph node metastasis (LNM) in the MRI results; when there is evidence of either or both of these factors, primary chemoradiation is selected. Assuming that this strategy is applied to our cohort, we evaluate how the rate of trimodality therapy is affected.
RESULTS
Of the 254 patients in our sample, 77 (30.3%) had at least one category 1 risk factor (PMI, LNM, positive resection margin) upon pathologic examination. If the MRI-based strategy had been applied to our cohort, 168 patients would have undergone primary surgery and 86 would have undergone primary chemoradiation. Only 25 patients (9.8%) would have required trimodality therapy based on an indication of at least one category 1 pathologic risk factor following radical hysterectomy.
CONCLUSION
The inclusion of MRI in the decision-making process for primary treatment modality could have reduced the number of patients requiring trimodality therapy based on the indication of a category 1 risk factor from 30.3% to 9.8% in our cohort.
Keyword
MeSH Terms
Figure
-
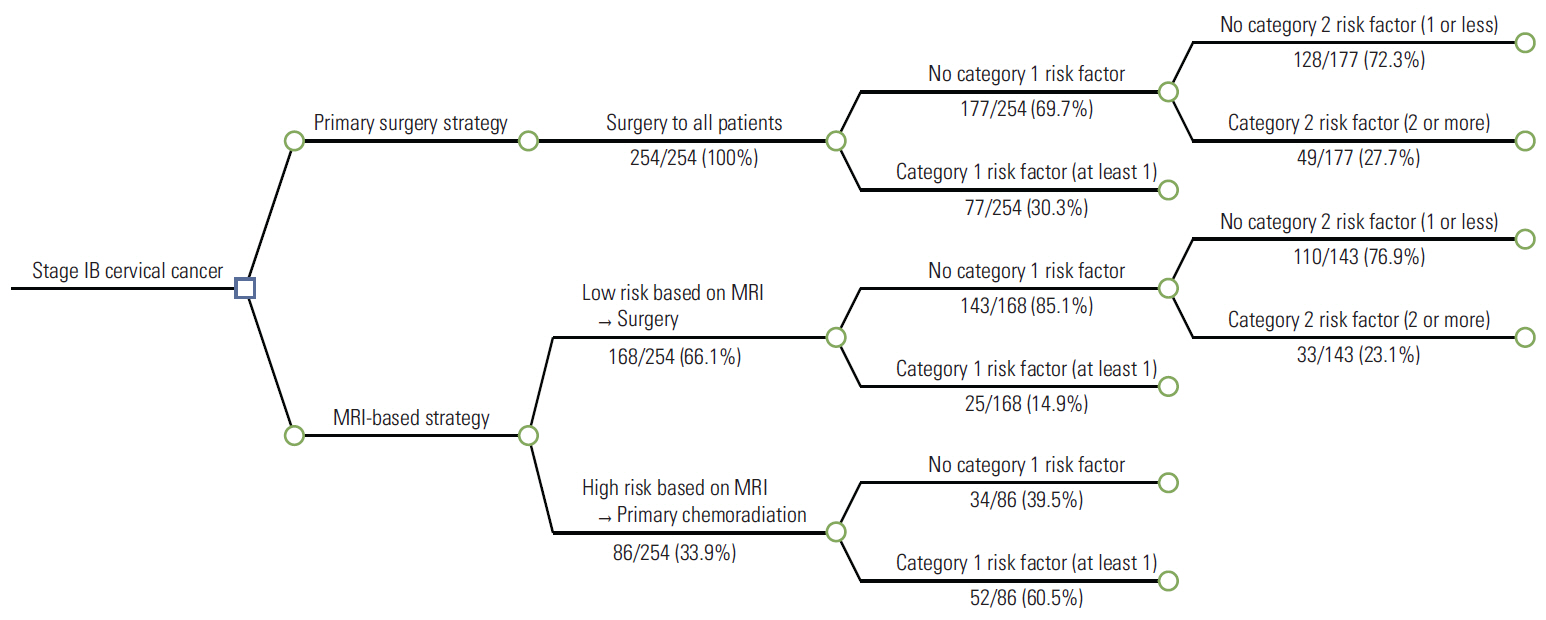
Fig. 1. A decision tree comparing the two strategies (primary surgery strategy and magnetic resonance imaging [MRI]–based strategy) for stage IB cervical cancer. Category 1 risk factors: positive resection margin, lymph node metastasis, parametrial involvement; category 2 risk factors: positive lymphovascular space invasion, deep stromal invasion, large tumor size.
Reference
-
References
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011; 61:69–90.
Article2. Jung KW, Won YJ, Kong HJ, Oh CM, Lee DH, Lee JS. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2011. Cancer Res Treat. 2014; 46:109–23.
Article3. Frumovitz M, Sun CC, Schover LR, Munsell MF, Jhingran A, Wharton JT, et al. Quality of life and sexual functioning in cervical cancer survivors. J Clin Oncol. 2005; 23:7428–36.
Article4. Schover LR, Fife M, Gershenson DM. Sexual dysfunction and treatment for early stage cervical cancer. Cancer. 1989; 63:204–12.
Article5. Barter JF, Soong SJ, Shingleton HM, Hatch KD, Orr JW Jr. Complications of combined radical hysterectomy-postoperative radiation therapy in women with early stage cervical cancer. Gynecol Oncol. 1989; 32:292–6.
Article6. Fiorica JV, Roberts WS, Greenberg H, Hoffman MS, LaPolla JP, Cavanagh D. Morbidity and survival patterns in patients after radical hysterectomy and postoperative adjuvant pelvic radiotherapy. Gynecol Oncol. 1990; 36:343–7.
Article7. Landoni F, Maneo A, Colombo A, Placa F, Milani R, Perego P, et al. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet. 1997; 350:535–40.
Article8. James RM, Cruickshank ME, Siddiqui N; Guideline Development Group. Management of cervical cancer: summary of SIGN guidelines. BMJ. 2008; 336:41–3.
Article9. Park JY, Kim DY, Kim JH, Kim YM, Kim YT, Kim YS, et al. Comparison of outcomes between radical hysterectomy followed by tailored adjuvant therapy versus primary chemoradiation therapy in IB2 and IIA2 cervical cancer. J Gynecol Oncol. 2012; 23:226–34.
Article10. Zivanovic O, Alektiar KM, Sonoda Y, Zhou Q, Iasonos A, Tew WP, et al. Treatment patterns of FIGO Stage IB2 cervical cancer: a single-institution experience of radical hysterectomy with individualized postoperative therapy and definitive radiation therapy. Gynecol Oncol. 2008; 111:265–70.
Article11. Amendola MA, Hricak H, Mitchell DG, Snyder B, Chi DS, Long HJ 3rd, et al. Utilization of diagnostic studies in the pretreatment evaluation of invasive cervical cancer in the United States: results of intergroup protocol ACRIN 6651/GOG 183. J Clin Oncol. 2005; 23:7454–9.
Article12. Goyal BK, Singh H, Kapur K, Duggal BS, Jacob MJ. Value of PET-CT in avoiding multimodality therapy in operable cervical cancer. Int J Gynecol Cancer. 2010; 20:1041–5.
Article13. Pandharipande PV, Choy G, del Carmen MG, Gazelle GS, Russell AH, Lee SI. MRI and PET/CT for triaging stage IB clinically operable cervical cancer to appropriate therapy: decision analysis to assess patient outcomes. AJR Am J Roentgenol. 2009; 192:802–14.
Article14. Lee JY, Youm J, Kim TH, Cho JY, Kim MA, Suh DH, et al. Preoperative MRI criteria for trials on less radical surgery in Stage IB1 cervical cancer. Gynecol Oncol. 2014; 134:47–51.
Article15. Jung DC, Kim MK, Kang S, Seo SS, Cho JY, Park NH, et al. Identification of a patient group at low risk for parametrial invasion in early-stage cervical cancer. Gynecol Oncol. 2010; 119:426–30.
Article16. National Comprehensive Cancer Center. Cervical cancer clinical practice guidelines in oncology (v.I.2014) [Internet]. Fort Washington, PA: National Comprehensive Cancer Center;2014 [cited 2014 Aug 4]. Available from: http://www.nccn.org.17. Capelle L, Stevens W, Brooks S. Patterns of care for cervical cancer in Auckland, New Zealand, 2003-2007. J Med Imaging Radiat Oncol. 2011; 55:82–9.
Article18. Ryu HS, Kang SB, Kim KT, Chang KH, Kim JW, Kim JH. Efficacy of different types of treatment in FIGO stage IB2 cervical cancer in Korea: results of a multicenter retrospective Korean study (KGOG-1005). Int J Gynecol Cancer. 2007; 17:132–6.
Article19. Galic V, Herzog TJ, Lewin SN, Neugut AI, Burke WM, Lu YS, et al. Prognostic significance of adenocarcinoma histology in women with cervical cancer. Gynecol Oncol. 2012; 125:287–91.
Article20. Lee JY, Kim YH, Kim MJ, Kim K, Chung HH, Park NH, et al. Treatment of stage IB2, IIA bulky cervical cancer: a single-institution experience of neoadjuvant chemotherapy followed by radical hysterectomy and primary radical hysterectomy. Arch Gynecol Obstet. 2011; 284:477–82.
Article21. Kim WY, Chang SJ, Chang KH, Yoo SC, Chun M, Ryu HS. Treatment patterns and outcomes in bulky stage IB2 cervical cancer patients: a single institution's experience over 14 years. Gynecol Obstet Invest. 2011; 71:19–23.
Article22. Rungruang B, Courtney-Brooks M, Beriwal S, Zorn KK, Richard SD, Olawaiye AB, et al. Surgery versus radiation therapy for stage IB2 cervical carcinoma: a population-based analysis. Int J Gynecol Cancer. 2012; 22:484–9.
Article23. Berveling MJ, Langendijk JA, Beukema JC, Mourits MJ, Reyners AK, Pras E. Health-related quality of life and late morbidity in concurrent chemoradiation and radiotherapy alone in patients with locally advanced cervical carcinoma. J Gynecol Oncol. 2011; 22:152–60.
Article24. Choi HJ, Ju W, Myung SK, Kim Y. Diagnostic performance of computer tomography, magnetic resonance imaging, and positron emission tomography or positron emission tomography/computer tomography for detection of metastatic lymph nodes in patients with cervical cancer: meta-analysis. Cancer Sci. 2010; 101:1471–9.
Article25. Marnitz S, Kohler C, Affonso RJ, Schneider A, Chiantera V, Tsounoda A, et al. Validity of laparoscopic staging to avoid adjuvant chemoradiation following radical surgery in patients with early cervical cancer. Oncology. 2012; 83:346–53.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The twenty-first century role of Piver-Rutledge type III radical hysterectomy and FIGO stage IA, IB1, and IB2 cervical cancer in the era of robotic surgery: a personal perspective
- The Role of Preoperative Breast MRI in Patients With Early-Stage Breast Cancer
- Minimally invasive radical hysterectomy and the importance of avoiding cancer cell spillage for early-stage cervical cancer: a narrative review
- Ovarian Metastasis from Stage IB Cervical Adenocarcinoma: A Case Report
- Predictive Value of Clinical Examination, Computed Tomography and Magnetic Resonance Imaging in the Clinical Staging of the Cervical Carcinoma
